


- Wakako Fujiwara Email author View ORCID ID profile,
- Tomohiro Haruki,
- Yoshiteru Kidokoro,
- Takashi Ohno,
- Yohei Yurugi,
- Ken Miwa,
- Yuji Taniguchi and
- Hiroshige Nakamura
Received: 28 March 2018
Accepted: 31 May 2018
Published: 11 June 2018
Abstract
Background
Ectopic ACTH-producing thymic carcinoid tumors are rare, but often behave aggressively with local invasion and distant metastasis. We herein report a case of ACTH-producing thymic typical carcinoid tumor with lymph node metastasis treated by surgery and postoperative radiation therapy.
Case presentation
A 61-year-old woman was admitted to be evaluated for hypoglycemia and hypokalemia. Laboratory data revealed elevation of serum cortisol and ACTH levels. Overnight administration of 8 mg dexamethasone did not suppress plasma ACTH. Chest CT demonstrated a tumor of 30 mm in diameter and enlargement of the lymph node at the anterior mediastinum. Ectopic ACTH syndrome was suspected and total thymectomy and lymph node dissection were performed. The histopathological examination indicated typical carcinoid tumor and mediastinal lymph node metastasis, and immunohistochemical staining was positive for ACTH. The plasma ACTH level decreased immediately after surgery. She received postoperative radiation therapy of 60 Gy.
Conclusion
Ectopic ACTH-producing thymic typical carcinoid tumors are rare, and it is important to consider this disease and perform appropriate treatment.
Keywords
Background
Among adrenocorticotrophic hormone (ACTH)-dependent Cushing’s syndrome, 10–20% is due to nonpituitary tumors termed ectopic ACTH syndrome (EAS). The most common cause of EAS is small cell lung cancer, followed by thymic carcinoids. Thymic carcinoids are very rare neuroendocrine tumors that often complicate endocrine disorders. Although previously assumed to be variants of bronchopulmonary carcinoid tumors, they are generally more aggressive and difficult to treat. It is widely accepted that surgical resection is the only curative treatment for localized lesions, and the efficacy of chemotherapy and radiotherapy has not been well established.
We herein report a case of EAS caused due to a thymic typical carcinoid tumor successfully treated by surgery followed by radiation.
Case presentation
A 61-year-old woman visited her primary care doctor because of general malaise, face edema, skin pigmentation, insomnia, and polyuria. Blood examination revealed marked hypokalemia and impaired glucose tolerance. Bilateral adrenal enlargement was observed on abdominal ultrasonography, and she was referred to our hospital for further examination. Endocrine examination showed both elevated plasma cortisol (107.7 pg/mL) and ACTH levels (1100 pg/mL), and increased urinary excretion of free cortisol (6650 mcg/day) and 17-ketogenic steroids (78.7 mg/day). Plasma cortisol and ACTH levels were elevated without any diurnal rhythm. Plasma cortisol was not suppressed by the overnight 8-mg dexamethasone suppression test. There was no response of plasma ACTH or cortisol to exogenous corticotropin-releasing hormone (CRH). Other hormones of the pituitary, thyroid, and adrenal medulla were all in normal ranges. Thus, ectopic ACTH syndrome was strongly suggested.
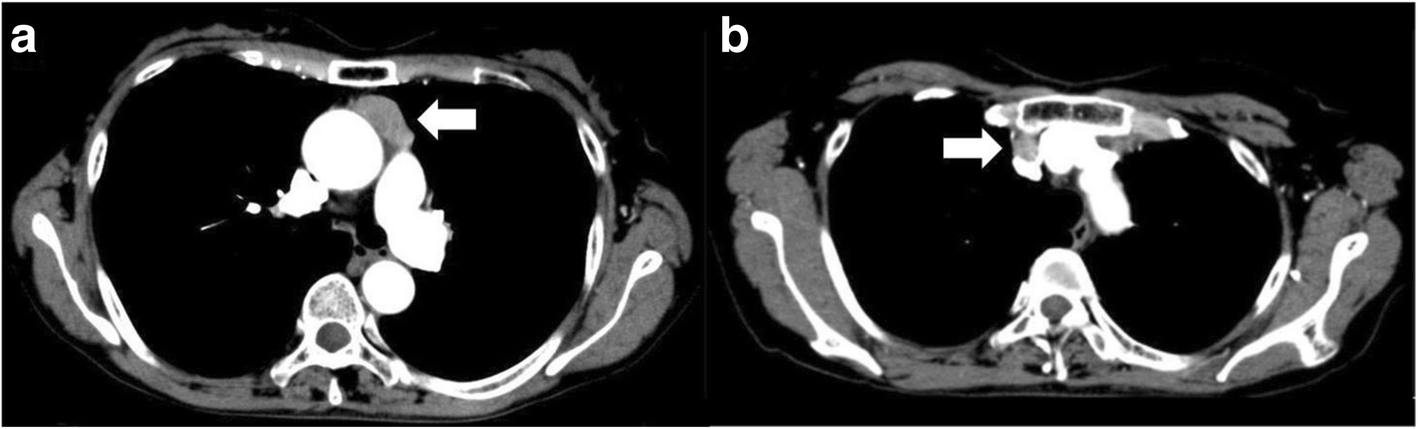
Chest CT image. A tumor (30 × 30 × 14 mm) without invasion localized in the anterior mediastinum (a). Enlargement of lymph node (b)
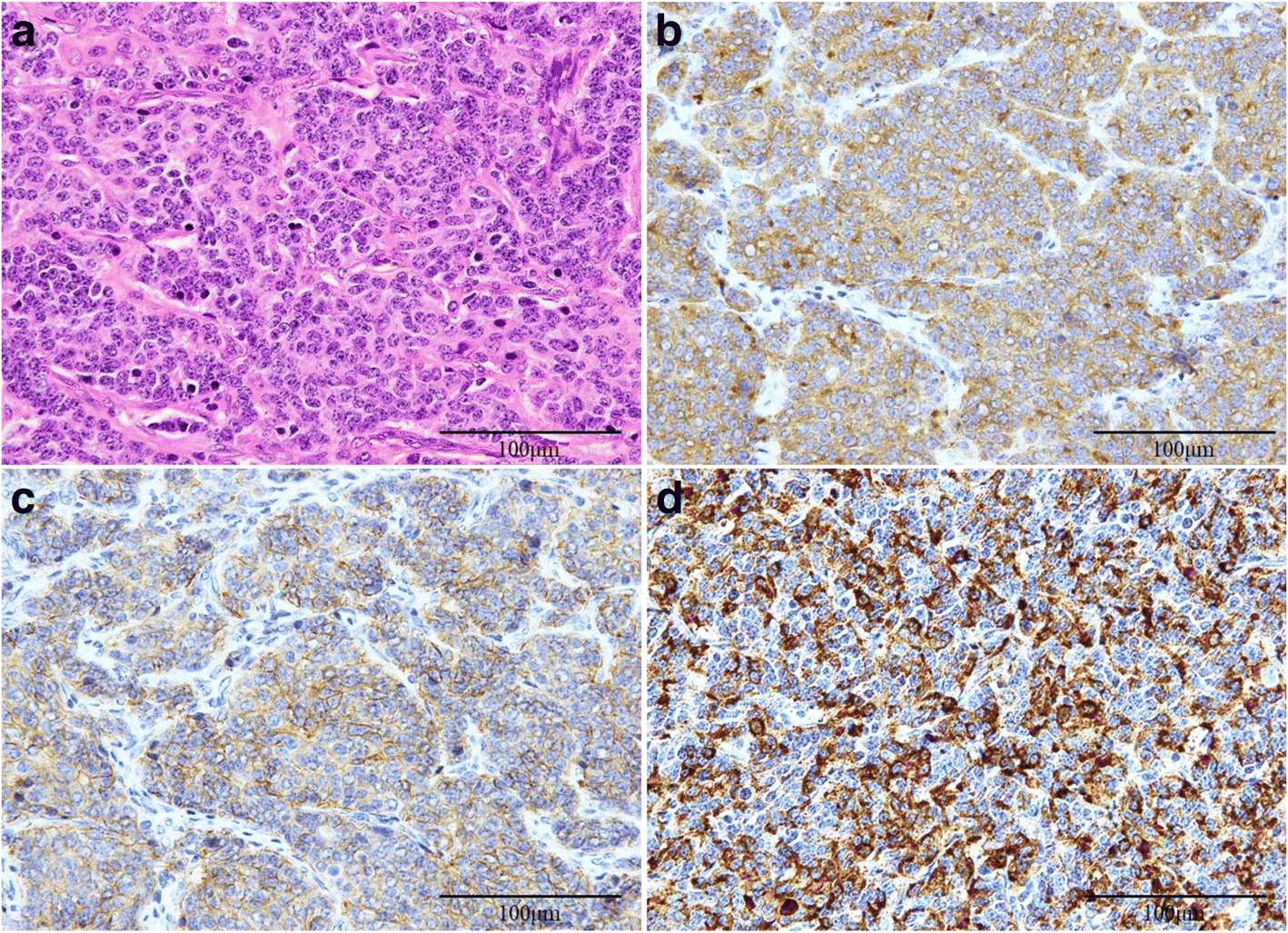
HE staining (a) indicated typical carcinoid tumor. Tumor cells were positive for synaptophysin (b), CD-56 (c), and ACTH (d) on immunostaining
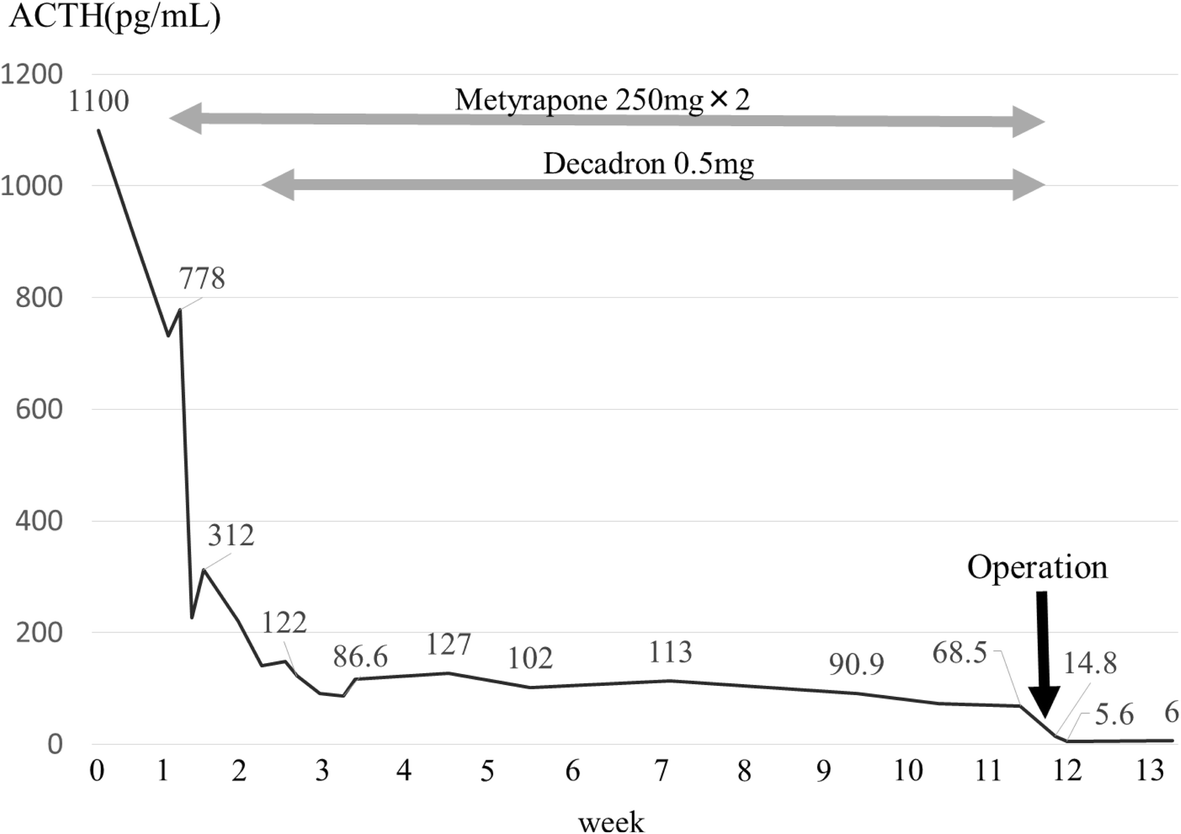
Changes in plasma ACTH levels during the clinical course
Discussion
Ectopic ACTH-producing thymic carcinoid tumor is an extremely rare clinical condition, comprising 29% of all thymic carcinoids and 5–42% of all ectopic ACTH-producing syndrome [1, 2]. It has been reported that radical surgical resection of the ACTH source is the only effective treatment [3]. Prior to surgery, medication therapy should be done to prevent perioperative complications and perform surgery when hormone values and symptoms are controlled. Furthermore, there is a risk of postoperative adrenal insufficiency; strict perioperative management is desirable.
Unlike pulmonary and other carcinoid tumors, thymic carcinoids often behave aggressively as an advanced disease with local invasion, lymph node metastasis, and distant metastasis because of the high proportion of atypical carcinoid tumors. Regarding ACTH-producing thymic tumors, Neary et al. reported three cases of well-differentiated ACTH-producing thymic neuroendocrine carcinomas, and the patients had no lymph node metastasis, recurrence, or death. On the other hand, nine cases of moderately differentiated ACTH-producing thymic neuroendocrine carcinomas almost had lymph node metastasis, and all patients had recurred [4]. However, our case was a typical carcinoid tumor with lymph node metastasis and local invasion.
As a surgical procedure, a median sternotomy approach is generally recommended because this enables excision of the entire thymus, perithymic fat, other affected mediastinal structure, and aggressive lymph node dissection. However, there is no standard for lymph node dissection in thymic epithelial tumors even though lymph node metastasis is an important prognostic factor. Hwang et al. recommended right paratracheal node dissection in addition to anterior regional lymph node dissection for TNM clinical stage II or higher diseases because they are crucial stations on the lymphatic pathway of thymic malignancies [5]. In the present case, we performed total thymectomy, followed by lymph node dissection of the anterior regional and right paratracheal nodes, and sampling of subcarinal lymph node via median sternotomy. The anterior mediastinal lymph nodes were positive for metastasis. Consequently, we considered the extent of lymph node dissection to be adequate, and radical resection was completed because the postoperative plasma ACTH level was successfully decreased. Although a good prognosis is expected by combined surgery and radiation, relatively high malignancy characteristics are observed compared with typical carcinoids, and strict follow-up is needed.
Conclusion
We report a rare case of ectopic ACTH-producing thymic typical carcinoid with local invasion and regional lymph node metastasis. Surgical resection was effective to control Cushing’s syndrome in this case, and nodal staging may help to guide adjuvant treatment, but systemic nodal dissection/sampling is yet to be standardized.
Abbreviations
- ACTH:
-
Adrenocorticotrophic hormone
- CRH:
-
Corticotropin-releasing hormone
- CT:
-
Computed tomography
- SUV:
-
Standardized uptake value
- PET:
-
Positron emission tomography
- MEN:
-
Multiple endocrine neoplasia
- HPF:
-
High-power fields
- CD-56:
-
Cluster of differentiation-56
Declarations
Acknowledgements
The authors thank Dr. Nosaka and Dr. Umekita for diagnostic assessment of this case.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article.
Authors’ contributions
WF and YT were the attending doctors for the patient. WF, YK, KM, YT, and HN performed the operation. WF, TH, and HN drafted this manuscript. All authors have read and approved the final manuscript.
Ethics approval and consent to participate
No applicable.
Consent for publication
This patient consented to the reporting of this case in a scientific publication.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
References
- Yoshikawa T, Noguchi Y, Matsukawa H, et al. Thymus carcinoid producing parathyroid hormone (PTH)-related protein: report of a case. Surg Today. 1994;24:544–7.View ArticlePubMedGoogle Scholar
- Alexandraki KI, Grossman AB. The ectopic ACTH syndrome. Rev Endocr Metab Disord. 2010;11:117–26.View ArticlePubMedGoogle Scholar
- Zhou X, Hnag J, Che J, et al. Surgical treatment of ectopic adrenocorticotropic hormone syndrome with intra-thoracic tumor. J Thorac Dis. 2016;8:888–93.View ArticlePubMedPubMed CentralGoogle Scholar
- Neary NM, Lopez-Chavez A, Abel BS, et al. Neuroendocrine ACTH-producing tumor of the thymus—experience with 12 patients over 25 years. J Clin Endocrinol Metab. 2012;97:2223–30.View ArticlePubMedPubMed CentralGoogle Scholar
- Hwang Y, Park IK, Park S, et al. Lymph node dissection in thymic malignancies: implication of the ITMIG lymph node map, TNM stage classification, and recommendations. J Thorac Oncol. 2016;11:108–14.View ArticlePubMedGoogle Scholar
Copyright
Filed under: adrenal, Cushing's, Rare Diseases | Tagged: abstract, ACTH, adrenal, Cushing's Syndrome, lymph nodes, radiation, thymectomy, thymic typical carcinoid |

Leave a comment