


Over the years, we went on several Windjammer Barefoot Cruises. We liked them because they were small, casual and were fairly easy on the wallet.
They sailed around the Caribbean to a variety of islands, although they sometimes changed itineraries depending on weather, crew, whatever. One trip we were supposed to go to Saba but couldn’t make port. A lot of people got off at the next port and flew home.
The captains were prone to “Bedtime Stories” which were often more fiction than true but they added to the appeal of the trip. We didn’t care if we missed islands or not – we were just there to sail over the waves and enjoy the ride.
The last trip we took with them was about two years before I started having Cushing’s problems. (You wondered how I was going to tie this together, right?)
The cruise was uneventful, other than the usual mishaps like hitting docks, missing islands and so on. Until it was a particularly rough sea one day. I was walking somewhere on deck and suddenly a wave came up over the deck making it very slippery. I fell and cracked the back of my head on the curved edge of a table in the dining area. I had the next-to-the-worse headache I have ever had, the worst being after my pituitary surgery. At least after the surgery, I got some morphine.
We asked several doctors later if that hit could have contributed to my Cushing’s but doctors didn’t want to get involved in that at all.
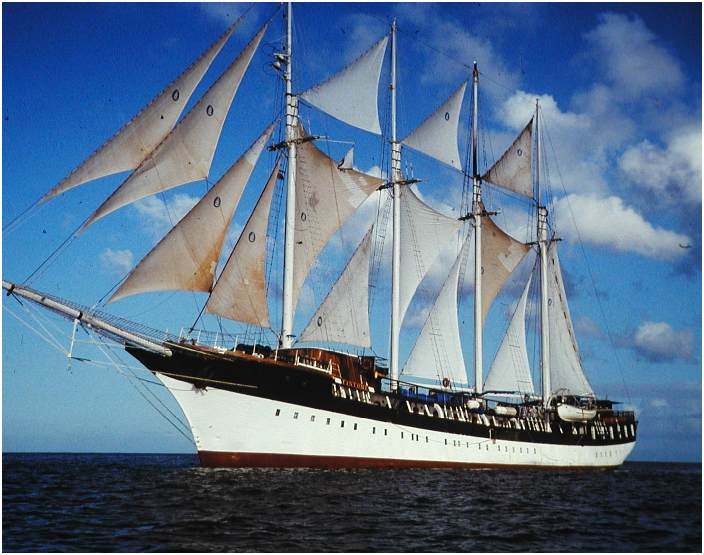
The Windjammer folks didn’t fare much better, either. In October 1998, Hurricane Mitch was responsible for the loss of the s/v Fantome (the last one we were on). All 31 crew members aboard perished; passengers and other crew members had earlier been offloaded in Belize.

The story was recorded in the book The Ship and the Storm: Hurricane Mitch and the Loss of the Fantome by Jim Carrier. The ship, which was sailing in the center of the hurricane, experienced up to 50-foot (15 m) waves and over 100 mph (160 km/h) winds, causing the Fantome to founder off the coast of Honduras.
“In October 1998, the majestic schooner Fantome came face-to-face with one of the most savage storms in Atlantic history. The last days of the Fantome are reconstructed in vivid and heartbreaking detail through Jim Carrier’s extensive research and hundreds of personal interviews. What emerges is a story of courage, hubris, the agony of command, the weight of lives versus wealth, and the advances of science versus the terrible power and unpredictability of nature.”
This event was similar to the Perfect Storm in that the weather people were more interested in watching the hurricane change directions than they were in people who were dealing with its effects.
I read this book and I was really moved by the plight of those crew members.
I’ll never know if that hit on my head contributed to my Cushing’s but I have seen several people mention on the message boards that they had a traumatic head injury of some type in their earlier lives.
Filed under: Cushing's | Tagged: Belize, cruise, Cushing's Awareness Challenge, Cushing's Awareness Challenge 2024, headache, Hurricane Mitch, MaryO, message boards, pituitary, surgery, Windjammer | Leave a comment »
