Background and purpose: Thymic neuroendocrine carcinomas (TNECs) are extremely uncommon. Certain cases of TNECs can produce the adrenocorticotropic hormone (ACTH) and cause ectopic ACTH syndrome (EAS). The current literature on this topic consists mainly of case reports, and therapeutic guidelines are lacking. The aim of this study was to discuss the diagnosis, surgical management, and prognosis of EAS caused by TNECs to improve clinical experience with this rare disease.
Methods: From June 1984 to June 2014, at the Peking Union Medical College Hospital, the surgical interventions and follow-up outcomes of 16 consecutive patients (eight men and eight women) with EAS caused by TNECs were retrospectively analyzed.
Results: The median age was 32.5 years (range: 13–47 years), and the median disease duration was 8.5 months (range: 1–150 months). All patients presented with clinical and biochemical evidence indicating a diagnosis of Cushing’s syndrome.
Contrast-enhanced thoracic computed tomography scans were critical to locating the ACTH-producing tumor and evaluating the feasibility of resection. All patients underwent surgery. One patient died of septicemia in the intensive care unit 2 weeks after surgery. No other morbidity or mortality occurred during the perioperative period. The median overall survival (OS) was 41 months (95% CI: 30.3–51.7 months), and the progression-free survival was 28 months (95% CI: 21.6–34.3 months). Both overall survival (P=0.002) and progression-free survival (P=0.030) improved significantly after complete resection.
Conclusion: TNEC is an extremely aggressive disease that should be considered when treating patients with Cushing’s syndrome due to ectopic ACTH secretion. In particular, all suspected patients should undergo contrast-enhanced thoracic computed tomography scans to facilitate early diagnosis. The current first-line treatment is surgical resection, and complete resection is a favorable prognostic factor. However, additional patients and a longer follow-up will be needed to determine the variables that are predictive of survival and to improve patient prognosis.
Over the years, we went on several Windjammer Barefoot Cruises. We liked them because they were small, casual and were fairly easy on the wallet.
They sailed around the Caribbean to a variety of islands, although they sometimes changed itineraries depending on weather, crew, whatever. One trip we were supposed to go to Saba but couldn’t make port. A lot of people got off at the next port and flew home.
The captains were prone to “Bedtime Stories” which were often more fiction than true but they added to the appeal of the trip. We didn’t care if we missed islands or not – we were just there to sail over the waves and enjoy the ride.
The last trip we took with them was about two years before I started having Cushing’s problems. (You wondered how I was going to tie this together, right?)
The cruise was uneventful, other than the usual mishaps like hitting docks, missing islands and so on. Until it was a particularly rough sea one day. I was walking somewhere on deck and suddenly a wave came up over the deck making it very slippery. I fell and cracked the back of my head on the curved edge of a table in the dining area. I had the next-to-the-worse headache I have ever had, the worst being after my pituitary surgery. At least after the surgery, I got some morphine.
We asked several doctors later if that hit could have contributed to my Cushing’s but doctors didn’t want to get involved in that at all.
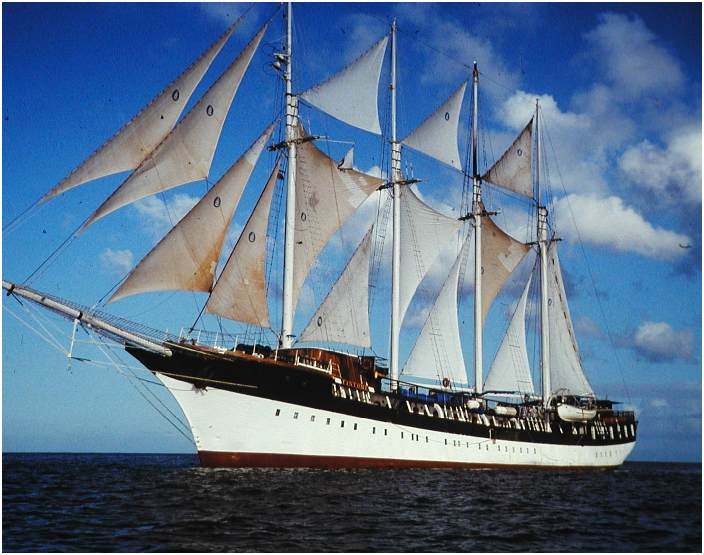
The Windjammer folks didn’t fare much better, either. In October 1998, Hurricane Mitch was responsible for the loss of the s/v Fantome (the last one we were on). All 31 crew members aboard perished; passengers and other crew members had earlier been offloaded in Belize.
The story was recorded in the book The Ship and the Storm: Hurricane Mitch and the Loss of the Fantome by Jim Carrier. The ship, which was sailing in the center of the hurricane, experienced up to 50-foot (15 m) waves and over 100 mph (160 km/h) winds, causing the Fantome to founder off the coast of Honduras.
“In October 1998, the majestic schooner Fantome came face-to-face with one of the most savage storms in Atlantic history. The last days of the Fantome are reconstructed in vivid and heartbreaking detail through Jim Carrier’s extensive research and hundreds of personal interviews. What emerges is a story of courage, hubris, the agony of command, the weight of lives versus wealth, and the advances of science versus the terrible power and unpredictability of nature.”
This event was similar to the Perfect Storm in that the weather people were more interested in watching the hurricane change directions than they were in people who were dealing with its effects.
I read this book and I was really moved by the plight of those crew members.
I’ll never know if that hit on my head contributed to my Cushing’s but I have seen several people mention on the message boards that they had a traumatic head injury of some type in their earlier lives.
In case you haven’t guessed it, my cause seems to be Cushing’s Awareness. I never really decided to devote a good portion of my life to Cushing’s, it just fell into my lap, so to speak – or my laptop.
I had been going along, raising my son, keeping the home-fires burning, trying to forget all about Cushing’s. My surgery had been a success, I was in remission, some of the symptoms were still with me but they were more of an annoyance than anything.
I started being a little active online, especially on AOL. At this time, I started going through real-menopause, not the fake one I had gone through with Cushing’s. Surprisingly, AOL had a group for Cushing’s people but it wasn’t very active.
What was active, though, was a group called Power Surge (as in I’m not having a hot flash, I’m having a Power Surge). I became more and more active in that group, helping out where I could, posting a few links here and there.
Around this time I decided to go back to college to get a degree in computer programming but I also wanted a basic website for my piano studio. I filled out a form on Power Surge to request a quote for building one. I was very surprised when Power Surge founder/webmaster Alice (AKA Dearest) called me. I was so nervous. I’m not a good phone person under the best of circumstances and here she was, calling me!
I had to go to my computer class but I said I’d call when I got back. Alice showed me how to do some basic web stuff and I was off. As these things go, the O’Connor Music Studio page grew and grew… And so did the friendship between Alice and me. Alice turned out to be the sister I never had, most likely better than any sister I could have had.
In July of 2000, Alice and I were wondering why there weren’t many support groups online (OR off!) for Cushing’s. This thought percolated through my mind for a few hours and I realized that maybe this was my calling. Maybe I should be the one to start a network of support for other “Cushies” to help them empower themselves.
I wanted to educate others about the awful disease that took doctors years of my life to diagnose and treat – even after I gave them the information to diagnose me. I didn’t want anyone else to suffer for years like I did. I wanted doctors to pay more attention to Cushing’s disease.
The first website (http://www.cushings-help.com) went “live” July 21, 2000. It was just a single page of information. The message boards began September 30, 2000 with a simple message board which then led to a larger one, and a larger. Today, in 2012, we have over 8 thousand members. Some “rare disease”!
This was on the intro page of Cushing’s Help until 2013…
I would like to give abundant thanks Alice Lotto Stamm, founder of Power Surge, premier site for midlife women, for giving me the idea to start this site, encouraging me to learn HTML and web design, giving us the use of our first spiffy chatroom, as well as giving me the confidence that I could do this. Alice has helped so many women with Power Surge. I hope that I can emulate her to a smaller degree with this site.
Thanks so much for all your help and support, Alice!
In August 2013 my friend died. In typical fashion, I started another website…
I look around the house and see things that remind me of Alice. Gifts, print outs, silly stuff, memories, the entire AOL message boards on floppy disks…
The resection of microadenomas — small, benign tumors in the pituitary gland underlying Cushing’s disease — could be aided by a fluorescent marker that is naturally produced by the tumor, a new study shows.
Cushing’s disease is characterized by high cortisol levels that cause debilitating physical, mental, and hormonal symptoms. The excess cortisol is caused by tiny benign tumors in the pituitary gland, called microadenomas, with a size of less than 10 millimeters.
On account of their small size, these microadenomas pose imaging challenges to physicians. Up to 40 percent of microadenomas remain undetected in the gold-standard magnetic resonance imaging (MRI).
Pituitary adenomas, however, have a characteristic that distinguishes them from the surrounding healthy tissue. They process (metabolize) a natural haemoglobin metabolite, called 5-aminolevulinic acid (5-ALA), into protoporphyrin IX (PpIX) at much higher rates — up to 20 to 50 times higher — than normal tissues.
Importantly, PpIX emits red fluorescence when excited with blue light.
This means that exogenous 5-ALA is taken up by the adenoma cells and rapidly metabolized into the fluorescent metabolite, PpIX, which may establish its use for fluorescence-guided resection of pituitary adenomas.
To test this, researchers incubated human-derived corticotropinoma, as well as the adjacent normal gland cells with 5-ALA. They did the same with mouse model normal pituitary cells and a mouse model pituitary tumor cell line, called AtT20.
They then analyzed the cells’ fluorescence profile by microscopy and with a technique called flow cytometry.
The analysis showed that compared to normal pituitary tissue, human-derived adenomatous cells had a significant increase of tenfold in 5-ALA-induced PpIX fluorescence intensity.
Similarly, mouse pituitary tumor cells (AtT20 cell line) fluoresced seven times more intensely than normal murine pituitary tissue.
The microscopy analysis revealed that the 5-ALA localized in subcellular organelles called mitochondria.
On June 6, 2017, the U.S. Food and Drug Administration approved the use of 5-ALA (under the brand name Gleolan) as an optical imaging agent for patients with gliomas (brain tumors), as an add-on compound to assist surgeons in identifying the malignant tissue during surgery.
Now, these findings suggest that 5-ALA also may be used for fluorescence-guided surgery of microadenomas in Cushing’s disease.
“The supraphysiological levels of glucocorticoids, as seen in CD [Cushing’s disease], may enhance the 5-ALA fluorescence in corticotropinomas,” researchers wrote.
It’s Sunday again, so this is another semi-religious post so feel free to skip it 🙂
I’m sure that many would think that Abide With Me is a pretty strange choice for my all-time favorite hymn.
My dad was a Congregational (now United Church of Christ) minister so I was pretty regular in church attendance in my younger years.
Some Sunday evenings, he would preach on a circuit and I’d go with him to some of these tiny churches. The people there, mostly older folks, liked the old hymns best – Fanny Crosby and so on.
So, some of my “favorite hymns” are those that I sang when I was out with my Dad. Fond memories from long ago.
In 1986 I was finally diagnosed with Cushing’s after struggling with doctors and trying to get them to test for about 5 years. I was going to go into the NIH (National Institutes of Health) in Bethesda, MD for final testing and then-experimental pituitary surgery.
I was terrified and sure that I wouldn’t survive the surgery.
Somehow, I found a 3-cassette tape set of Readers Digest Hymns and Songs of Inspiration and ordered that. The set came just before I went to NIH and I had it with me.
At NIH I set up a daily “routine” of sorts and listening to these tapes was a very important part of my day and helped me get through the ordeal of more testing, surgery, post-op and more.
When I had my kidney cancer surgery, those tapes were long broken and irreplaceable, but I had replaced all the songs – this time on my iPod.
Abide With Me was on this original tape set and it remains a favorite to this day. Whenever we have an opportunity in church to pick a favorite, my hand always shoots up and I request page 700. When someone in one of my handbell groups moves away, we always sign a hymnbook and give it to them. I sign page 700.
I think that many people would probably think that this hymn is depressing. Maybe it is but to me it signifies times in my life when I thought I might die and I was so comforted by the sentiments here.
This hymn is often associated with funeral services and has given hope and comfort to so many over the years – me included.
If you abide in Me, and My words abide in you, you will ask what you desire, and it shall be done for you.
~John 15:7
Abide With Me
Words: Henry F. Lyte, 1847.
Music: Eventide, William H. Monk, 1861. Mrs. Monk described the setting:
This tune was written at a time of great sorrow—when together we watched, as we did daily, the glories of the setting sun. As the last golden ray faded, he took some paper and penciled that tune which has gone all over the earth.
Lyte was inspired to write this hymn as he was dying of tuberculosis; he finished it the Sunday he gave his farewell sermon in the parish he served so many years. The next day, he left for Italy to regain his health. He didn’t make it, though—he died in Nice, France, three weeks after writing these words. Here is an excerpt from his farewell sermon:
O brethren, I stand here among you today, as alive from the dead, if I may hope to impress it upon you, and induce you to prepare for that solemn hour which must come to all, by a timely acquaintance with the death of Christ.
For over a century, the bells of his church at All Saints in Lower Brixham, Devonshire, have rung out “Abide with Me” daily. The hymn was sung at the wedding of King George VI, at the wedding of his daughter, the future Queen Elizabeth II, and at the funeral of Nobel peace prize winner Mother Teresa of Calcutta in1997.
Abide with me; fast falls the eventide;
The darkness deepens; Lord with me abide.
When other helpers fail and comforts flee,
Help of the helpless, O abide with me.
Swift to its close ebbs out life’s little day;
Earth’s joys grow dim; its glories pass away;
Change and decay in all around I see;
O Thou who changest not, abide with me.
Not a brief glance I beg, a passing word;
But as Thou dwell’st with Thy disciples, Lord,
Familiar, condescending, patient, free.
Come not to sojourn, but abide with me.
Come not in terrors, as the King of kings,
But kind and good, with healing in Thy wings,
Tears for all woes, a heart for every plea—
Come, Friend of sinners, and thus bide with me.
Thou on my head in early youth didst smile;
And, though rebellious and perverse meanwhile,
Thou hast not left me, oft as I left Thee,
On to the close, O Lord, abide with me.
I need Thy presence every passing hour.
What but Thy grace can foil the tempter’s power?
Who, like Thyself, my guide and stay can be?
Through cloud and sunshine, Lord, abide with me.
I fear no foe, with Thee at hand to bless;
Ills have no weight, and tears no bitterness.
Where is death’s sting? Where, grave, thy victory?
I triumph still, if Thou abide with me.
Hold Thou Thy cross before my closing eyes;
Shine through the gloom and point me to the skies.
Heaven’s morning breaks, and earth’s vain shadows flee;
RSS Error: A feed could not be found at `http://www.oconnormusic.org/feed.xml`; the status code is `503` and content-type is `text/html; charset=us-ascii`
RSS Error: A feed could not be found at `http://www.oconnormusic.org/bios.xml`; the status code is `503` and content-type is `text/html; charset=us-ascii`