Early diagnosis and immediate treatment of Cushing’s syndrome (CS) are critical for a better prognosis but remain a challenge. However, few comprehensive reports have focused on this issue or investigated whether patient-reported manifestations are consistent with physician-assessed symptoms of CS. This study aimed to clarify the differences in patient-reported and physician-assessed manifestations of signs and symptoms of CS that prevent early diagnosis.
Methods
This single-center retrospective study included 52 patients with CS (16 with Cushing’s disease and 36 with adrenal CS). Upon clinical diagnosis, medical records were used to independently review the patient-reported and physician-assessed manifestations of typical (such as purple striae and proximal myopathy) and nonspecific features (such as hirsutism and hypertension). The correlations and differences between the patient-reported and physician-assessed manifestations were then analyzed.
Results
We observed a positive correlation between the total number of manifestations of nonspecific features reported by patients and those assessed by physicians, but not for typical features. Moreover, manifestations reported by the patients were less frequent than those assessed by physicians for typical features, leading to discrepancies between the two groups. In contrast, there were no differences in most nonspecific features between the patient-reported and physician-assessed manifestations. Notably, the concordance between patient-reported and physician-assessed manifestations of typical features was not associated with urinary free cortisol levels.
Conclusion
Regardless of disease severity, patients often do not complain of the typical features of CS that are crucial for formulating a diagnosis.
Introduction
Endogenous Cushing’s syndrome (CS) is caused by chronic and excessive glucocorticoid exposure. This occurs primarily due to adrenocorticotropic hormone (ACTH)-producing pituitary tumors (Cushing’s disease; CD) or cortisol-producing adrenal tumors (adrenal Cushing’s syndrome; ACS) [1]—and has a high mortality rate owing to cardiovascular disease, severe infection, and suicide, even when diagnosed and treated appropriately [1, 2]. Moreover, the prognosis is poor if the disease is not adequately treated or remains undiagnosed [2]. Therefore, early diagnosis and immediate intervention are important, as remission of CS due to surgical and pharmacological treatment can reduce the risk of mortality [3, 4].
CS is a rare disease with a prevalence of 57 per million individuals and an annual incidence of 3.2 per million, and its epidemiology is consistent across various regions worldwide [5, 6]. Most symptoms and signs of CS are common in general metabolic disorders, including obesity, hypertension, osteoporosis, and diabetes mellitus [7]. However, CS should be suspected if these symptoms appear as unusual features for their age [1, 8]. Consequently, the identification of CS is challenging and labor-intensive [1, 9, 10]. In fact, recent research revealed that a definitive diagnosis of CD (the most common form of CS), took an average of 3.8 ± 4.8 years from the onset of symptoms, and patients typically consulted 4.6 ± 3.8 medical professionals before this disease was identified [11]. Typical features of CS include symptoms of moon face, central obesity, or buffalo hump [12], which are similar to other symptoms such as primary obesity and therefore can lead to misdiagnosis. Furthermore, although purple striae or thin skin with an increased propensity for bruising are other typical features of CS [12], these attributes are not commonly acknowledged by the general population [1, 9].
Anzeige
Attempts have been made to diagnose CS early, including the development of scoring systems to estimate the pre-test probability of CS and facial image analysis software to diagnose the specific facial features of CS [13‐15]; however, these have not yet been used widespread or fully and the early diagnosis of CS remains dependent on the experience-based medical skills of the clinical staffs [16].
Additionally, although it is difficult for patients to recognize complex and nonspecific symptoms [17, 18], the significance of patients recognizing their illness has recently been reported for various diseases such as heart failure and malignant carcinoma [19‐21]. It is widely acknowledged that patients’ self-recognition can result in early detection of the disease, reduce its severity and recurrence, and enhance their quality of life [19]. In patients with endocrine diseases, there is increasing focus on issues surrounding self-recognition [22‐24]. For example, a previous study focusing on acromegaly reported a discrepancy between patient-reported and physician-reported manifestations and indicated that resolving this discrepancy could shorten the time to diagnosis [25].
Identifying CS may be challenging for primary care physicians who are yet to specialize. Therefore, endocrinologists with extensive experience in CS have often noticed that patients and these physicians struggle to identify the symptoms of CS; however, few comprehensive reports have focused on this issue or investigated whether patient-reported manifestations are consistent with physician-assessed symptoms of CS.
Therefore, this study aimed to investigate the unreported manifestations of CS among individuals referred to non-specialist healthcare providers, including primary care physicians, and to recognize potential challenges with the current diagnosis of CS with the goal of facilitating early detection.
Anzeige
Materials and methods
Patients, study design, and data collection
This single-center retrospective study was conducted to identify the discrepancies between patient-reported and physician-assessed symptoms and investigate the factors causing these differences.
From September 2004 to December 2022, 199 patients were referred to our department at a tertiary medical institution upon suspicion, evaluation, or follow-up for hypercortisolism. Of these patients, 92 were newly diagnosed with CS (36 with CD, 51 with ACS, and 5 with ectopic ACTH syndrome) based on the diagnostic guidelines [3, 8, 12], with a diagnosis confirmed by pathological evaluation after surgical resection [26]. However, 35 patients were excluded due to a lack of detailed clinical data on the manifestations at diagnosis. Similarly, we excluded individuals diagnosed with ectopic ACTH syndrome because of the lack of comprehensive information on symptoms reported by the patients and primary care physicians due to the rapid progression and severity of this disease. Therefore, 52 patients (16 with CD and 36 with ACS) were enrolled in this study.
Upon clinical diagnosis, the manifestations included in the comprehensive standardized interview at the time of diagnosis and those assessed by the physician through collaborative assessment with multiple board-certified endocrinologists as routine practice were independently reviewed from the medical records. We categorized these manifestations reviewed from the medical records into the following two categories based on the diagnostic guidelines including those of the Japan Endocrine Society: typical features, including moon face, central obesity or buffalo hump, purple striae of ≥1 cm, thin skin and easy bruising, and proximal myopathy; and nonspecific features (shown as atypical in Japan Endocrine Society’s guideline), including hypertension, menstrual abnormalities, acne, hirsutism, peripheral edema, glucose metabolism impairment, osteoporosis, pigmentation (which is not expected in patients with ACS), and mental abnormalities [1, 8, 12]. Central obesity or buffalo hump can also be observed in pseudo CS. However, in this study, features were classified as the same typical feature according to clinical guidelines [12, 27]. We also reviewed the biochemical findings, comorbidities, duration from the initial recognition of CS-related symptoms to diagnosis, and number of medical institutions visited before diagnosis.
The present retrospective study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Kobe University Hospital (Approval No. 1351). The patients had the option of an opt-out process, and all procedures were part of routine medical care.
Definition of patient-reported and physician-assessed manifestations
In the context of routine clinical care, physicians asked the patients about the presence or absence of manifestations and comorbidities (e.g., hypertension, menstrual abnormalities, glucose metabolism impairment, osteoporosis, and mental abnormalities), which were documented in the medical records. These reports in the medical records were defined as patient-reported manifestations in this study. In contrast, the manifestations and comorbidities of CS were assessed within several weeks after the patient was referred to our department for suspected CS. Additional diagnostic information on comorbidities is provided in the subsequent section. Physician-assessed manifestations were subsequently defined based on these findings.
Comorbidities of Cushing’s syndrome
All comorbidities were diagnosed according to the appropriate guidelines [28‐30]. For example, hypertension was diagnosed if patients were taking oral antihypertensive medication or had more than grade 1 hypertension (≥140/90 mmHg) in a treatment-naïve state [28]. Moreover, glucose metabolism impairment—including diabetes mellitus, impaired glucose tolerance, and impaired fasting glucose—was diagnosed based on the results of blood glucose levels during fasting and after a 75-g oral glucose tolerance test, as well as hemoglobin A1c (HbA1c) levels [29]. Patients taking medications for diabetes mellitus at the time of CS diagnosis were also categorized as having diabetes.
Other comorbidities included mental abnormalities, menstrual abnormalities, and the presence of osteoporosis. Mental abnormalities were defined as the use of anxiolytic medications, sleeping pills, or antidepressants prescribed by experienced psychologists, and menstrual abnormalities were defined as women with irregular menstrual cycles. Furthermore, the presence of osteoporosis was defined as bone mineral density (BMD) of <–2.5 standard deviations (SD) of the T-score of the lumbar vertebrae (L2–L4), femoral neck, or distal radius measured using dual-energy x-ray absorptiometry (DXA; Horizon A DXA System), and/or an experience of a fragility fracture [30]. As per the specifications of the measurement system employed, L1 was not included in the assessment. The Z-score was also employed as a diagnostic reference among young adults. Patients also diagnosed with osteoporosis who were receiving medications for this disease.
Hormone assay
In this study, blood samples were collected after an overnight fast. Subsequently, serum cortisol levels were measured using a chemiluminescent enzyme immunoassay [CLEIA] (TOSOH, Tokyo, Japan, RRID:AB_3099658) or enzyme immunoassay [EIA] (TOSOH, Tokyo, Japan, RRID:AB_3076600). Similarly, plasma ACTH levels were measured using a CLEIA (TOSOH, Tokyo, Japan, RRID:AB_3099657, or Siemens, Tokyo, Japan, RRID:AB_2909441) and EIA (TOSOH, Tokyo, Japan, RRID:AB_2783633). In both methods, the measurements showed good correlation and no conversion was required [31, 32].
Anzeige
Urinary free cortisol (UFC) levels were also measured using radioimmunoassays (RIA; TFB, Tokyo, Japan, RRID:AB_2894408) or chemiluminescent immunoassays (CLIA; Siemens, Tokyo, Japan, RRID:AB_2893154). Using the following formula, the UFC levels measured by RIA were then corrected to the value measured by CLIA: Y = 0.832X − 4.23 (Y = UFC levels using CLIA, X = UFC levels using RIA) [33].
Statistical analysis
All statistical analyses were performed using SPSS ver. 28.0 software (IBM Corp., Armonk, NY, USA). All continuous variables were analyzed using the Shapiro–Wilk normality test to confirm a normal distribution, whereas Fisher’s exact test was used to analyze categorical data. Between the two groups, differences in normally or non-normally distributed data were compared using the unpaired Student’s t-test or the Mann–Whitney U test, respectively.
Cohen’s kappa coefficient was used to describe the concordance between the patient-reported and physician-assessed manifestations. As previously reported [19, 20, 34], the concordance based on the value of Cohen’s kappa coefficient was rated as follows: 0.00–0.20 for “Slight,” 0.21–0.40 for “Fair,” 0.41–0.60 for “Moderate,” 0.61–0.80 for “Substantial,” and 0.81–1.00 for “Almost Perfect.” For correlation analysis between two variables of non-normally distributed data, we used Spearman’s rank correlation coefficient. Multivariate logistic regression analyses were then performed to investigate variables associated with the discrepancies between patient-reported and physician-assessed manifestations.
The results are presented as mean ± SD for normally distributed data and median [interquartile range] for non-normally distributed data, and differences were considered statistically significant when the P value was <0.05.
Anzeige
Results
Clinical characteristics of the patients
We included 52 patients diagnosed with CS in this study. Their clinical characteristics are presented in Table 1. Notably, this group consisted of 5 males and 47 females, with a mean age of 49.4 ± 15.8 years, median body mass index (BMI) of 23.0 [21.3–28.0] kg/m2, and median UFC level of 272.1 [126.0–435.0] µg/day. Of the CS patients, 16 had CD and 36 had ACS, which is consistent with epidemiological data on CS observed in Asians (including Japanese individuals); however, this differed from epidemiological data from Western countries [35, 36]. Regarding comorbidities, 43 patients were diagnosed with hypertension—of which 34 were prescribed antihypertensive medications—with a mean systolic blood pressure (BP) of 136.4 ± 21.5 mmHg and diastolic BP of 83.5 ± 15.0 mmHg. In addition, 44 patients were diagnosed with glucose metabolism impairment—of which, 20 were prescribed oral hypoglycemic agents and/or insulin—with a median fasting serum glucose level of 99.5 [87.3–116.5] mg/dL and median HbA1c level of 6.3% [5.7–7.4]. Moreover, 29 patients were diagnosed with osteoporosis, of which 4 were prescribed antiosteoporosis medication, with BMD T-score SDs of -1.54 ± 1.39, -1.76 ± 1.12, and -0.50 [-1.53–0.50] for the lumber spine, femoral neck, and distal radius, respectively. Notably, the UFC levels were higher in patients with CD than in those with ACS (412.6 [243.2–1,100.3] vs. 215.3 [114.0–387.8] µg/day); however, there were no significant differences attributed to sex, age, BMI, or the proportion of patients with respect to comorbidities, including hypertension and glucose metabolism impairment, between patients with CD and ACS.
Table 1
Clinical characteristics of the patients
Total
CD
ACS
CD vs. ACS P value
Number of men/women
5/47
1/15
4/32
1.00
Age (years)
49.4 ± 15.8
54.3 ± 19.2
47.2 ± 13.8
0.14
BMI (kg/m2)
23.0 [21.3–28.0]
24.7 [22.2–30.0]
22.8 [20.8–26.4]
0.17
Midnight F (µg/dL)
20.1 [16.0–23.5]
20.2 [13.9–24.7]
20.1 [16.9–23.0]
0.97
F after LDDST (μg/dL)
21.2 ± 6.9
24.2 ± 10.1
19.7 ± 4.2
0.11
UFC (μg/day)
272.1 [126.0–435.0]
412.6 [243.2–1,100.3]
215.3 [114.0–387.8]
0.02
Basal ACTH (pg/mL)
2.0 [0.0–53.9]
83.2 [57.4–169.9]
0.0 [0.0–2.1]
<0.01
Systolic BP (mmHg)
136.4 ± 21.5
140.5 ± 20.7
134.6 ± 21.8
0.36
Diastolic BP (mmHg)
83.5 ± 15.0
83.1 ± 14.3
83.6 ± 15.5
0.90
Use of antihypertensive drugs, n (%)
34 (65)
13 (81)
21 (58)
0.13
FSG (mg/dL)
99.5 [87.3–116.5]
110.0 [102.0–142.8]
92.5 [83.3–114.3]
0.01
HbA1c (%)
6.3 [5.7–7.4]
6.8 [5.9–8.6]
6.0 [5.7–7.1]
0.08
Use of OHA and/or insulin, n (%)
20 (38)
9 (56)
11 (31)
0.12
LS BMD T-score (SD)
−1.54 ± 1.39
−1.00 ± 1.38
−1.79 ± 1.35
0.07
LS BMD Z-score (SD)
−0.78 ± 1.37
0.13 ± 1.11
−1.20 ± 1.28
<0.01
FN BMD T-score (SD)
−1.76 ± 1.12
−1.73 ± 1.54
−1.78 ± 0.88
0.92
FN BMD Z-score (SD)
−0.79 ± 1.01
−0.39 ± 1.10
−0.99 ± 0.92
0.10
Radius BMD T-score (SD)
−0.50 [−1.53–0.50]
−0.30 [−2.50–0.40]
−0.60 [−1.30–0.60]
0.79
Radius BMD Z-score (SD)
0.60 [−0.60–1.50]
1.50[−0.60–1.80]
0.50[−0.50–1.00]
0.33
Use of antiosteoporosis drugs, n (%)
4 (8)
1 (6)
3 (8)
1.00
Time to diagnosis (months)
44.0 [13.3–125.3]
43.0 [15.0–128.3]
47.5 [12.5–125.3]
0.87
Number of medical institutions before diagnosis
3.0 [2.0–5.0]
3.0 [2.0–5.0]
3.0 [3.0–5.8]
0.23
The results are presented as mean ± SD for normally distributed data and median [interquartile range] for non-normally distributed data
CD Cushing’s disease, ACS adrenal Cushing’s syndrome, BMI body mass index, F cortisol, LDDST low-dose dexamethasone suppression test, UFC urinary free cortisol, ACTH adrenocorticotropic hormone, BP blood pressure, FSG fasting serum glucose, HbA1c hemoglobin A1c, OHA oral hypoglycemic agents, BMD bone mineral density, LS lumber spine, FN femoral neck
The median duration from the patients’ initial recognition of CS-related manifestations to diagnosis was 44.0 [13.3–125.3] months, and it took more than 3 years to diagnose CS in 30 patients (58%). Furthermore, the median number of medical facilities visited by patients before diagnosis was 3.0 [2.0–5.0]; however, there were no significant differences in the duration or number of medical institutions between patients with CD and those with ACS.
Frequency and concordance between patient-reported and physician-assessed CS-related manifestations
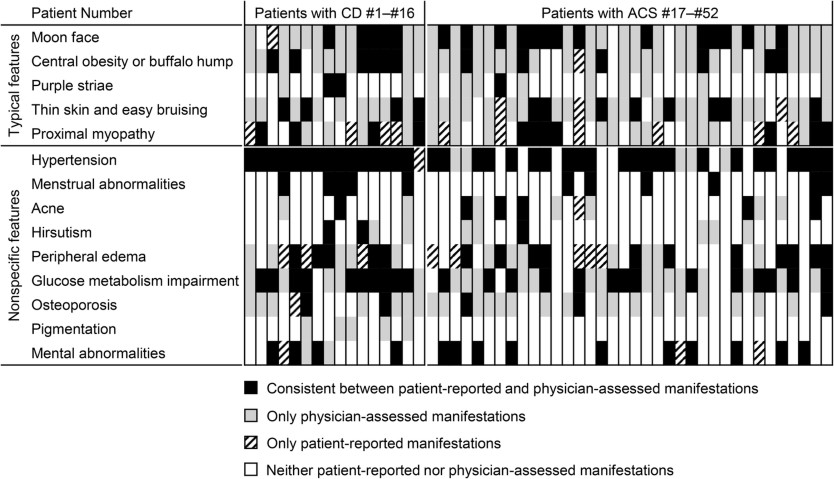
Each manifestation reported by a patient or assessed by a physician is shown vertically for individual cases in Fig. 1. Compared with nonspecific features, typical features appeared to not be reported by the patients but were only assessed by the physicians. In addition, compared to nonspecific features, there were fewer cases in which the manifestations reported by the patients were consistent with those assessed by physicians for typical features.
Fig. 1
Consistency between patient-reported and physician-assessed manifestations for each individual case. The consistencies or discrepancies between patient-reported and physician-assessed manifestations are shown. Vertical lines represent manifestations in individual patients. CD Cushing’s disease, ACS adrenal Cushing’s syndrome
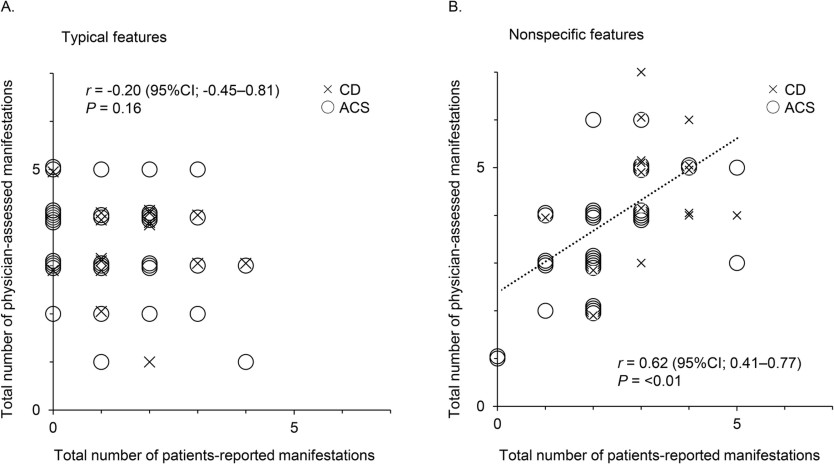
Consistent with the impact of these visually distinctive presentations shown in Fig. 1, no correlation was observed in the number of typical features between patient-reported and physician-assessed manifestations (r = –0.20, P = 0.16) (Fig. 2A), whereas a positive correlation was found for nonspecific features (r = 0.62, P < 0.01) (Fig. 2B). Moreover, the total number of patient-reported manifestations of typical features was lower than that of physician-assessed manifestations (1.0 [0.0–2.0] vs. 3.5 [3.0–4.0], P < 0.01), and four of the five typical features were reported less frequently by patients than by physicians, except for proximal myopathy (Table 2A). According to Cohen’s kappa coefficient, the concordance between patient-reported and physician-assessed manifestations was marked as “Fair” to “Slight,” indicating a discrepancy for all typical features. Similarly, the total number of patient-reported manifestations of nonspecific features was also lower than that in physicians (2.5 [2.0–3.0] vs. 4.0 [3.0–5.0], P < 0.01). However, except for glucose metabolism impairment or osteoporosis, there were no differences in the frequencies of nonspecific features between patient-reported and physician-assessed manifestations, and the concordance of the nonspecific features between the patient-reported and physician-assessed manifestations was “Almost perfect” for menstrual abnormality and “Substantial” for mental abnormality and hypertension, whereas that for glucose metabolism impairment and osteoporosis was “Fair.” This suggests that the discrepancy between patient-reported and physician-assessed manifestations was more significant for typical than for nonspecific features. However, no differences in these discrepancies were observed between patients with CD and those with ACS (Table 2B, C).
Fig. 2
Correlation between the total number of patient-reported and physician-assessed manifestations. Correlations between the total number of patient-reported and physician-assessed manifestations are shown for typical (A) and nonspecific features (B). CD is plotted by ×, and ACS is plotted by ○. The Spearman’s rank correlation coefficients and P value are presented. CI confidence interval, CD Cushing’s disease, ACS adrenal Cushing’s syndrome
Table 2
Frequencies of patient-reported and physician-assessed manifestations and their concordance. A. All patients (n = 52). B. Patients with CD (n = 16). C. Patients with ACS (n = 36)
Patient-reported
Physician-assessed
P value of Fisher’s exact test
Concordance with Cohen’s kappa coefficient
A
Typical features
Moon face, n (%)
20 (39)
48 (92)
<0.01
Slight
Central obesity or buffalo hump, n (%)
13 (25)
44 (85)
<0.01
Slight
Purple striae, n (%)
3 (6)
15 (29)
<0.01
Fair
Thin skin and easy bruising, n (%)
15 (29)
43 (83)
<0.01
Slight
Proximal myopathy, n (%)
21 (40)
27 (52)
0.33
Slight
Nonspecific features
Hypertension, n (%)
39 (75)
43 (83)
0.47
Substantial
Menstrual abnormalities, n (%)
11 (21)
11 (21)
1.00
Almost perfect
Acne, n (%)
7 (14)
13 (25)
0.21
Moderate
Hirsutism, n (%)
3 (6)
10 (19)
0.07
Moderate
Peripheral edema, n (%)
24 (46)
28 (54)
0.56
Fair
Glucose metabolism impairment, n (%)
24 (46)
44 (85)
<0.01
Fair
Osteoporosis, n (%)
7 (14)
29 (56)
<0.01
Slight
Pigmentation, n (%)
0 (0)
5 (10)
0.06
–
Mental abnormalities, n (%)
17 (33)
17 (33)
1.00
Substantial
B
Typical features
Moon face, n (%)
6 (38)
14 (88)
0.01
Slight
Central obesity or buffalo hump, n (%)
6 (38)
15 (94)
<0.01
Slight
Purple striae, n (%)
2 (13)
4 (25)
0.56
Moderate
Thin skin and easy bruising, n (%)
4 (25)
13 (81)
0.06
Slight
Proximal myopathy, n (%)
8 (50)
8 (50)
1.00
Slight
Nonspecific features
Hypertension, n (%)
16 (100)
15 (94)
0.78
Slight
Menstrual abnormalities, n (%)
5 (31)
5 (31)
1.00
Almost perfect
Acne, n (%)
1 (6)
3 (19)
0.56
Moderate
Hirsutism, n (%)
2 (13)
4 (25)
0.56
Moderate
Peripheral edema, n (%)
8 (50)
10 (63)
0.56
Slight
Glucose metabolism impairment, n (%)
10 (63)
15 (94)
0.14
Slight
Osteoporosis, n (%)
4 (25)
9 (56)
0.15
Slight
Pigmentation, n (%)
0 (0)
5 (31)
0.14
–
Mental abnormalities, n (%)
5 (31)
6 (38)
0.78
Moderate
C
Typical features
Moon face, n (%)
14 (39)
34 (94)
<0.01
Slight
Central obesity or buffalo hump, n (%)
7 (19)
29 (81)
<0.01
Slight
Purple striae, n (%)
1 (3)
11 (31)
<0.01
Slight
Thin skin and easy bruising, n (%)
11 (31)
30 (83)
<0.01
Slight
Proximal myopathy, n (%)
13 (36)
19 (53)
0.24
Slight
Nonspecific features
Hypertension, n (%)
23 (64)
28 (78)
0.30
Substantial
Menstrual abnormalities, n (%)
6 (17)
6 (17)
1.00
Almost perfect
Acne, n (%)
6 (17)
10 (28)
0.40
Moderate
Hirsutism, n (%)
1 (3)
6 (17)
0.11
Fair
Peripheral edema, n (%)
16 (44)
18 (50)
0.81
Fair
Glucose metabolism impairment, n (%)
14 (39)
29 (81)
<0.01
Fair
Osteoporosis, n (%)
3 (8)
20 (56)
<0.01
Slight
Pigmentation, n (%)
0 (0)
0 (0)
–
–
Mental abnormalities, n (%)
12 (33)
11 (31)
1.00
Almost perfect
The frequencies of patient-reported and physician-assessed manifestations were compared using Fisher’s exact test. The concordance between patient-reported and physician-assessed manifestations was evaluated with Cohen’s kappa coefficient, and its coefficients were defined as follows: 0.00–0.20 for “Slight,” 0.21–0.40 for “Fair,” 0.41–0.60 for “Moderate,” 0.61–0.80 for “Substantial,” and 0.81–1.00 for “Almost perfect”
CD Cushing’s disease, ACS adrenal Cushing’s syndrome
Anzeige
We performed logistic regression analyses using UFC to investigate whether excess cortisol levels influenced the discrepancy between patient-reported and physician-assessed manifestations. Notably, we observed no association between UFC levels and discrepancies between patient-reported and physician-assessed manifestations in the univariate or multivariate logistic regression analyses adjusted for sex and age (Table 3A). In addition, no association was observed after adjusting for other variables such as BMI and disease duration. Similarly, we found that the serum cortisol levels after the low-dose dexamethasone suppression test (LDDST) were not associated with discrepancies between patient-reported and physician-assessed manifestations (Table 3B). Thus, these disparities were shown to be insignificant when directly related to the severity of CS.
Table 3
Logistic regression analyses of the discrepancies between the patient-reported and physician-assessed manifestations. A. Variables associated with UFC levels. B. Variables associated with serum cortisol levels after the LDDST
Univariate
Multivariate 1 (sex- and age-adjusted)
Multivariate 2 (BMI-adjusted)
Multivariate 3 (disease duration-adjusted)
A
Moon face
1.000 (0.999–1.001)
1.000 (0.999–1.001)
1.000 (0.998–1.002)
1.000 (0.999–1.001)
Proximal myopathy
1.000 (0.999–1.001)
1.000 (0.999–1.001)
1.000 (0.998–1.001)
1.000 (0.998–1.001)
Thin skin and easy bruising
1.000 (0.998–1.001)
1.000 (0.999–1.001)
1.000 (0.999–1.001)
1.000 (0.998–1.001)
Central obesity or buffalo hump
1.001 (1.000–1.003)
1.001 (1.000–1.003)
1.001 (1.000–1.003)
1.001 (1.000–1.003)
Purple striae
1.000 (0.999–1.002)
1.000 (0.998–1.002)
1.001 (0.999–1.003)
1.000 (0.999–1.002)
B
Moon face
0.998 (0.919–1.084)
0.999 (0.919–1.086)
1.000 (0.920–1.088)
0.997 (0.918–1.082)
Proximal myopathy
1.007 (0.925–1.097)
1.007 (0.924–1.097)
1.007 (0.925–1.097)
1.006 (0.924–1.096)
Thin skin and easy bruising
1.022 (0.939–1.112)
1.018 (0.934–1.109)
1.023 (0.940–1.113)
1.019 (0.937–1.109)
Central obesity or buffalo hump
0.979 (0.890–1.078)
0.978 (0.865–1.105)
0.981 (0.875–1.099)
0.978 (0.887–1.078)
Purple striae
0.998 (0.919–1.084)
0.999 (0.919–1.086)
1.000 (0.920–1.088)
0.997 (0.918–1.082)
The results are presented as odds ratios (95% confidence intervals)
UFC urinary free cortisol, BMI Body Mass Index, LDDST low-dose dexamethasone suppression test
Discussion
In the present study, we highlight the challenges associated with the diagnosis of CS—a condition resulting from excessive glucocorticoid exposure—and elucidate the divergence between patient-reported and physician-assessed manifestations. Thus, this study may aid in the early detection of CS by identifying symptoms that patients are unable to recognize based on the disparities between patient-reported and physician-assessed manifestations of CS.
In this study, the number of patient-reported manifestations of both typical and nonspecific features was lower than that of physician-assessed manifestations, suggesting that CS symptoms may have been overlooked by relying solely on patient reports. Additionally, analysis of the concordance between patient-reported and physician-assessed manifestations revealed a tendency for these manifestations to be inconsistent for both typical and nonspecific features, with a tendency to be more significant for typical features. Furthermore, the UFC and serum cortisol levels after the LDDST, which represent the severity of CS, were not associated with the concordance of manifestations between patients and physicians, suggesting that even in cases of severe CS, patients may not recognize their symptoms. These findings imply that typical features, which are essential for diagnosing CS, may be difficult for patients to recognize and poorly identified or conveyed to patients by non-specialist physicians, who are typically the first to interact with individuals with CS. The importance of educating healthcare providers such as primary care physicians, family physicians and gynecologists for early diagnosis of CS should be highlighted.
According to a previous report on the diagnostic history of 176 patients with CD, 83% of the patients visited their family physician for manifestations such as weight gain and hypertension, while 46% visited a gynecologist for menstrual abnormalities before the diagnosis of CD [11]. Thus, the typical features of CS were not recognized. The examination may reveal nonspecific features. However, individuals who are non-specialists may not recognize these features as indications of CS. Therefore, patients are often unaware of the potential complications associated with CS. This is consistent with the results of our study, in which patient-reported and physician-assessed manifestations were more consistent for hypertension and menstrual abnormalities than for other manifestations such as typical features, glucose metabolism impairment, and osteoporosis. This makes diagnosis challenging as non-specialist physicians and, more prominently, patients may not recognize the full range of symptoms associated with CS, especially the typical features with high diagnostic value. In addition, older patients diagnosed with CS present with a lower BMI and waist circumference than younger patients [37], and they typically do not exhibit symptoms commonly associated with CS such as skin alterations, depression, hair loss, hirsutism, and reduced libido. These findings may further complicate the diagnosis of CS in elderly patients.
By evaluating only the patient-reported manifestations, it appears that manifestations such as peripheral edema and proximal myopathy were more common. Possibly, these symptoms were not considered features of CS by physicians, in comparison to the degree of symptoms experienced by the patients. However, this may not necessarily imply diminishing the significance of the patient’s signs and symptoms, as these manifestations can be considered as the unidentified complaints and may result in a postponement of the diagnosis of CS. Patients may be experiencing symptoms that physicians do not perceive, indicating the importance of interview and physical examination. Further investigation is needed to elucidate underlying factors.
Considering the rarity of CS, it is crucial to suspect and diagnose the condition based on clinical symptoms and perform the appropriate screening tests without over- or under-screening [7]. Although CS screening in patients with diabetes mellitus and hypertension has been reported to lead to a diagnosis in only 0–0.7% and 0.1–0.5% of these patients, respectively [38‐41], it is ineffective in terms of false positives and cost [9]. Therefore, patients with typical features that are highly specific for CS, such as purple striae, easy bruising, and proximal myopathy [1, 8, 12], as well as those with obesity, diabetes mellitus, or hypertension in combination with these features, should be screened for CS [7, 27]. However, our results suggest that these symptoms are unlikely to be self-recognized. Therefore, the appropriate screening measures must be implemented to establish an early and effective diagnosis of CS.
In these situations, it is crucial for physicians to utilize their knowledge and experience to suspect CS based on symptoms such as typical features [10]. It has been reported that years of clinical experience in endocrine practice can contribute to the estimation of the pre-test probability of CS [16]. In contrast, non-specialists are less likely to encounter patients with CS in their lifetime, which can make it difficult to properly suspect CS [9]. From this perspective, it is of utmost importance that family physicians and general internists are knowledgeable regarding the manifestations that require screening for CS, as early diagnosis of this uncommon and severe condition is crucial [11]. Therefore, it is important for physicians who routinely treat patients presenting with common symptoms such as obesity, diabetes mellitus, and hypertension to meticulously interview and observe for any indicators of CS, even if the patient does not recognize them. Failure to adopt an appropriate tone in these situations may cause the disease to become undetectable.
In rare disorders such as CS, in addition to enhancing public recognition of the disease, the appropriate sharing of information and provision of specialized care in clinical practice remain important issues [42]. Early identification of such rare diseases can be achieved by promoting an understanding of the disease and its symptoms among family, friends, and patients who may be the first to recognize the signs and symptoms in an individual. In fact, in a questionnaire survey of 340 patients with CS across 30 countries, the diagnosis of CS was made in 5.6% of cases by the patients themselves and in 0.9% by their family or friends [43]. In the present study, we found that it took more than 3 years to diagnose CS in 58% of the cases. If CS and its symptoms are popularized among the public, the typical features of CS could be more readily reported to physicians and the time to diagnosis might be shorter. Furthermore, a primary care physician who is well-educated and knowledgeable is crucial in ensuring that the concerns of such individuals are not overlooked.
This study has some limitations. First, this single-center retrospective study included a relatively small sample size with few male patients. Second, CD and ACS have different pathologies; therefore, the frequencies of several CS-related manifestations will differ depending on their subtypes [3, 44]. However, in this study, there was no difference in the discrepancies between patient-reported and physician-assessed manifestations in patients with CD or ACS. Nonetheless, it is crucial that comprehensive research is conducted in larger patient populations with a focus on employing methods that accurately reflect the pathophysiology of CD and ACS. Third, patient reports may be inaccurate in terms of onset and duration because they depend on the patient’s memory. Fourth, the endocrinologists who examined the patients differed, which may have affected the presence or absence of physician-assessed manifestations. Finally, this study investigated the differences between the manifestations reported by patients and those assessed by endocrinologists, although the evaluations conducted by primary care physicians, which are crucial for the early detection of CS, were not available. Future research is needed to investigate the differences in recognizing manifestations between non-specialist physicians and endocrinologists with extensive experience in CS and to examine the changes before and after education for these non-specialists to determine if they can lead to earlier diagnosis of CS.
In conclusion, endocrinologists have been shown to be aware of CS-related symptoms, especially typical features, whereas patients do not recognize these manifestations, even when the disease is severe. Therefore, the key to the early diagnosis and treatment of CS is a more proactive approach of questioning and examining patients suspected of having the disease.
Acknowledgements
We thank all the physicians and medical assistants who were involved in this study. We are grateful to all the laboratory members for their excellent discussions and fruitful suggestions. We also thank Editage (www.editage.jp) for English language editing.
Compliance with ethical standards
Conflict of interest
The authors declare no competing interests.
Ethics approval
This study conformed to the Declaration of Helsinki guidelines and was approved by the Ethics Committee of Kobe University Hospital (Approval No. 1351).
Informed consent
Informed consent was obtained from all the participants using an opt-out approach.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
There is increasing evidence that multisystem morbidity in patients with Cushing’s disease (CD) is only partially reversible following treatment. We investigated complications from multiple organs in hospitalized patients with CD compared to patients with non-functioning pituitary adenoma (NFPA) after pituitary surgery.
Design
Population-based retrospective cohort study using data from the Swiss Federal Statistical Office between January 2012 and December 2021.
Methods
Through 1:5 propensity score matching, we compared hospitalized patients undergoing pituitary surgery for CD or NFPA, addressing demographic differences. The primary composite endpoint included all-cause mortality, major adverse cardiac events (i.e., myocardial infarction, unstable angina, heart failure, cardiac arrest, ischemic stroke), hospitalization for psychiatric disorders, sepsis, severe thromboembolic events, and fractures in need of hospitalization. Secondary endpoints comprised individual components of the primary endpoint and surgical reintervention due to disease persistence or recurrence.
Results
After matching, 116 patients with CD (mean age 45.4 years [SD, 14.4], 75.0% female) and 396 with NFPA (47.3 years [14.3], 69.7% female) were included and followed for a median time of 50.0 months (IQR 23.5, 82.0) after pituitary surgery. CD presence was associated with a higher incidence rate of the primary endpoint (40.6 vs. 15.7 events per 1,000 person-years, HR 2.75; 95% CI, 1.54 to 4.90). CD patients also showed increased hospitalization rates for psychiatric disorders (HR 3.27; 95% CI, 1.59 to 6.71) and a trend for sepsis (HR 3.15; 95% CI, 0.95 to 10.40).
Conclusions
Even after pituitary surgery, CD patients faced a higher hazard of complications, especially psychiatric hospitalizations and sepsis.
Accepted manuscripts are PDF versions of the author’s final manuscript, as accepted for publication by the journal but prior to copyediting or typesetting. They can be cited using the author(s), article title, journal title, year of online publication, and DOI. They will be replaced by the final typeset articles, which may therefore contain changes. The DOI will remain the same throughout.
Spontaneous remission of Cushing’s disease (CD) is uncommon and often attributed to pituitary tumor apoplexy. We present a case involving a 14-year-old female who exhibited clinical features of Cushing’s syndrome. Initial diagnostic tests indicated CD: elevated 24h urinary cortisol (235 µg/24h, n < 90 µg/24h), abnormal 1 mg dexamethasone overnight test (cortisol after 1 mg dex 3.4 µg/dL, n < 1.8 µg/dL), and elevated adrenocorticotropic hormone concentrations (83.5 pg/mL, n 10-60 pg/mL). A pituitary adenoma was suspected, so a nuclear MRI was performed, with findings suggestive of a pituitary microadenoma. The patient was referred for a transsphenoidal resection of the microadenoma. While waiting for surgery, the patient presented to the emergency department with a headache and clinical signs of meningism. A computed axial tomography of the central nervous system was performed, and no structural alterations were found. The symptoms subsided with analgesia. One month later, she presented again to the emergency department with clinical findings of acute adrenal insufficiency (cortisol level of 4.06 µg/dL), and she was noted to have spontaneous biochemical remission associated with the resolution of her symptoms of hypercortisolism. For that reason, spontaneous CD remission induced by pituitary apoplexy (PA) was diagnosed. The patient has been managed conservatively since the diagnosis and remains in clinical and biochemical remission until the present time, after 10 months of follow-up. There are three unique aspects of our case: the early age of onset of symptoms, the spontaneous remission of CD due to PA, which has been rarely reported in the medical literature, and the fact that the patient presented a microadenoma because there are fewer than 10 clinical case reports of PA associated with microadenoma.
Introduction
Cushing’s disease (CD) is characterized by excessive production of adrenocorticotropic hormone by a pituitary adenoma and represents the most common cause of endogenous Cushing’s syndrome (CS) [1]. CD was first reported in 1912 by Harvey Williams Cushing, and he described 12 cases at the Peter Bent Brigham Hospital in Baltimore [2]. This disease has a global incidence of approximately 2.2 cases per 1,000,000 people and occurs more frequently in women from 20 to 50 years of age [3]. Pituitary apoplexy (PA) is a rare condition that occurs in 2-12% of cases, and it has a high morbidity and mortality rate [4]. We report an interesting case of a woman diagnosed with CD who achieved spontaneous remission of her disease after a PA.
Case Presentation
A 14-year-old female presented with a two-year history of weight gain (32 kg), depression, elevated blood pressure, type 2 diabetes mellitus, and growth failure (height less than the third percentile). Her height was 140 cm, and her BMI was 28.1 (97th percentile). At presentation, she had not yet reached menarche. Physical examination revealed Tanner 2 breast development, acne, hirsutism, moon facies, dorsocervical fat pad, central obesity, and stretch marks. Initial laboratory tests showed hemoglobin A1C of 13%, low-density lipoprotein of 167 mg/dL, triglycerides of 344 mg/dL, high-density lipoprotein of 26 mg/dL, creatinine of 0.4 mg/dL, and elevated liver enzymes. Abdominal ultrasound indicated moderate hepatic steatosis changes.
Given the high suspicion of CS, a hormonal profile was conducted (Table 1), confirming CS and subsequently diagnosing CD. A nuclear MRI revealed a 2.6 × 1.8 mm pituitary lesion (Figure 1), prompting referral for transsphenoidal resection of the pituitary microadenoma.
Laboratories
Reference range
Initial
One month
Three months
Six months
TSH (mUI/L)
0.35-4.94
–
2.17
–
2.01
AM cortisol (µg/dL)
6.02-18.4
17.3
4.06
<0.5
4.7
1 mg DST (µg/dL)
<1.8
3.4
–
–
–
8 mg DST (µg/dL)
<50% suppression
1.9 (78% suppression)
–
–
–
Urine-free cortisol (µg/24h)
<90
235
–
–
–
ACTH (pg/mL)
10-60
83.5
–
19.2
9.7
IGF-1 (ng/mL)
36-300
–
–
–
293
Table 1: Pertinent laboratory investigation at baseline and follow-up with our patient
Figure 1: Axial view of a T1 MRI with contrast showing a sellar lesion
The red arrow shows a microadenoma in relation to the normal pituitary gland.
Approximately one month after the suppression tests and while awaiting surgery, the patient presented to the emergency department with a sudden, severe, holocranial headache accompanied by projectile vomiting and diplopia, suggestive of meningism. A computed axial tomography of the central nervous system was conducted, revealing no structural abnormalities. Symptoms resolved with intravenous analgesia within approximately four to six hours. Subsequently, the patient experienced a significant decrease in insulin requirements, ultimately leading to the suspension of insulin therapy due to persistent hypoglycemia.
Weeks after the headache episode, the patient was reevaluated in the emergency department with a three-day history of diffuse abdominal pain, vomiting, asthenia, myalgia, hypotension, tachycardia, orthostatism, and recurrent hypoglycemia despite insulin suspension. Acute adrenal insufficiency was suspected and confirmed by a cortisol level of 4.06 µg/dL. Treatment with intravenous hydrocortisone 50 mg every six hours was initiated, leading to complete resolution of symptoms within 72 hours. The patient was discharged on maintenance therapy with oral hydrocortisone (20 mg in the morning and 10 mg at night). Subsequent follow-ups showed undetectable cortisol levels. Currently, the patient has been followed up for 10 months post-event, showing persistent clinical and hormonal remission of her disease.
Discussion
CD represents approximately 80% of cases of endogenous hypercortisolism, and pituitary microadenomas are the most common cause of CD in all age groups [5]. CD prevalence is 0.3-6.2 cases per 100,000 people [3], which represents 4.4% of all pituitary adenomas [6], and it is up to five times more likely to occur in women than men. Spontaneous remission of CD is rare, and it is mainly due to the apoplexy of a pituitary tumor [7].
PA is a potentially fatal condition resulting from hemorrhage or necrosis of a pituitary adenoma that produces compression of the surrounding structures with symptoms that can be critical and even fatal [8]. PA affects between 2% and 12% of patients with pituitary adenomas, mainly in nonfunctional macroadenomas [9]. Although the main mechanism of PA is hemorrhage, it can also be due to a hemorrhagic infarction or an infarction without hemorrhage; this last scenario is clinically less aggressive [10]. Among the most important precipitating factors are craniocerebral trauma, pregnancy, thrombocytopenia, coagulopathies, pituitary stimulation tests, drugs such as anticoagulants and estrogens, surgeries that are complicated by hypotension, and radiotherapy [4,11,12].
There are three unique aspects of our case. First, the age of onset is 14 years old. This characteristic has been reported in less than 6% of cases of CD, with a mean age of onset between 12.3 and 14.1 years and a slightly higher incidence in men (63%) [13]. In this population, CD is the most common cause of hypercortisolism, accounting for 75-80% of all cases [14]. Furthermore, our patient presented a significant weight gain, severe compromise in her height, hypertension, depression, and diabetes mellitus, which is compatible with the classic profile described for CD in pediatric ages. It is important to clarify that although type 2 diabetes mellitus is common in adults, it is unusual in the pediatric population [13].
Second, spontaneous remission in CD due to apoplexy has been rarely reported in the past; hence, our case is an important addition to the scant literature on this unusual phenomenon. Although there are characteristics suggestive of PA, such as hyperdense lesions within the pituitary gland and the reinforcing ring, a CT scan has a low sensitivity for detecting pituitary hemorrhage (21-46%); therefore, a negative CT scan does not rule out PA in cases where there is infarction without hemorrhage, a situation that could correspond to our case [15].
The third unique feature of our case is that the stroke occurred in the context of a microadenoma, a situation reported in less than 10 cases in the literature. Despite being a microadenoma, the symptoms of PA were severe, with symptoms of meningism, an intense headache, vomiting, and the development of adrenal insufficiency. Taylor et al. [16] reported a similar case of a 41-year-old female with microadenoma whose PA was associated with severe headache and vomiting.
The main differential diagnosis in our case is cyclical CS (CCS), a disorder that occurs in 15% of CS cases, especially in CD [17]. The diagnosis of CCS is classically established with three peaks and two valleys in cortisol secretion, spontaneous fluctuations, and clinical features of CS [7]. The possibility of CCS was ruled out due to the typical presentation of the PA event and the persistence of hypocortisolism.
Finally, several cases of recurrence of their disease have been described after remission of CS due to AP. Those recurrences usually develop in follow-ups of up to seven years [18]. At the time of the last evaluation (10 months post-PA), the patient remained in remission, but long-term follow-up is required to detect both reactivation and hypopituitarism [19].
Conclusions
CD is a rare entity in the pediatric population, usually associated with a pituitary microadenoma. Spontaneous remission of this disease is very uncommon, but when it occurs, it is mainly due to PA. We describe a case with three unique aspects: CD with an early age of onset of symptoms, spontaneous remission of CD due to PA, which has been rarely reported in the medical literature, and the fact that there are less than 10 clinical case reports of PA associated with microadenoma. It is imperative for clinicians to be aware of this possible outcome in patients with CD.
Cushing syndrome (CS) is a rare endocrinological disorder resulting from chronic exposure to excessive cortisol. The term Cushing disease is used specifically when this is caused by excessive secretion of adrenocorticotropic hormone (ACTH) by a pituitary tumor, usually an adenoma. This disease is associated with a poor prognosis, and if left untreated, it has an estimated 5-year survival rate of 50%. We present the case of a 66-year-old female patient who received a referral to endocrinology for an evaluation of obesity due to right knee arthropathy. Taking into consideration her age, she was screened for osteoporosis, with results that showed diminished bone density. Considering this, combined with other clinical features of the patient, suspicion turned toward hypercortisolism. Laboratory findings suggested that the CS was ACTH-dependent and originated in the pituitary gland. After a second look at the magnetic resonance imaging results, a 4-mm lesion was identified on the pituitary gland, prompting a transsphenoidal resection of the pituitary adenoma.
Chronic excessive exposure to glucocorticoids leads to the diverse clinical manifestations of Cushing syndrome (CS), which has an annual incidence ranging from 1.8 to 3.2 cases per million individuals [1]. The syndrome’s signs and symptoms are not pathognomonic, and some of its primary manifestations, such as obesity, hypertension, and glucose metabolism alterations, are prevalent in the general population [2], making diagnosis challenging. Endogenous CS falls into 2 categories: adrenocorticotropic hormone (ACTH)-dependent (80%-85% of cases), mostly due to a pituitary adenoma, or ACTH-independent (15%-20% of cases), typically caused by adrenal adenomas or hyperplasia [3]. Cushing disease (CD) represents a specific form of CS, characterized by the presence of an ACTH-secreting pituitary tumor [1]. Untreated CD is associated with high morbidity and mortality compared to the general population [1], with a 50% survival rate at 5 years [2]. However, surgical removal of a pituitary adenoma can result in complete remission, with mortality rates similar to those of the general population [2]. This article aims to highlight the challenges of suspecting and diagnosing CD and to discuss the current management options for this rare condition.
Case Presentation
A 66-year-old woman received a referral to endocrinology for an evaluation of obesity due to right knee arthropathy. During physical examination, she exhibited a body mass index of 34.3 kg/m2, blood pressure of 180/100, a history of non-insulin-requiring type 2 diabetes mellitus with glycated hemoglobin (HbA1c) of 6.9% (nondiabetic: < 5.7%; prediabetic: 5.7% to 6.4%; diabetic: ≥ 6.5%) and hypertension. Additionally, the patient complained of proximal weakness in all 4 limbs.
Diagnostic Assessment
Upon admission, densitometry revealed osteoporosis with T scores of −2.7 in the lumbar spine and −2.8 in the femoral neck. Hypercortisolism was suspected due to concomitant arterial hypertension, central obesity, muscle weakness, and osteoporosis. Physical examination did not reveal characteristic signs of hypercortisolism, such as skin bruises, flushing, or reddish-purple striae. Late-night salivary cortisol (LNSC) screening yielded a value of 8.98 nmol/L (0.3255 mcg/dL) (reference value [RV] 0.8-2.7 nmol/L [0.029-0.101 mcg/dL]) and ACTH of 38.1 pg/mL (8.4 pmol/L) (RV 2-11 pmol/L [9-52 pg/mL]). A low-dose dexamethasone suppression test (LDDST) was performed (cutoff value 1.8 mcg/dL [49 nmol/L]), with cortisol levels of 7.98 mcg/dL (220 nmol/L) at 24 hours and 20.31 mcg/dL (560 nmol/L) at 48 hours. Subsequently, a high-dose dexamethasone suppression test (HDDST) was conducted using a dose of 2 mg every 6 hours for 2 days, for a total dose of 16 mg, revealing cortisol levels of 0.0220 nmol/L (0.08 ng/mL) at 24 hours and 0.0560 nmol/L (0.0203 ng/mL) at 48 hours, alongside 24-hour urine cortisol of 0.8745 nmol/L (0.317 ng/mL) (RV 30-145 nmol/24 hours [approximately 11-53 μg/24 hours]) [4].
These findings indicated the presence of endogenous ACTH-dependent hypercortisolism of pituitary origin. Consequently, magnetic resonance imaging (MRI) was requested, but the results showed no abnormalities. Considering ectopic ACTH production often occurs in the lung, a high-resolution chest computed tomography scan was performed, revealing no lesions.
Treatment
Upon reassessment, the MRI revealed a 4-mm adenoma, prompting the decision to proceed with transsphenoidal resection of the pituitary adenoma.
Outcome and Follow-Up
The histological analysis revealed positive staining for CAM5.2, chromogranin, synaptophysin, and ACTH, with Ki67 staining at 1%. At the 1-month follow-up assessment, ACTH levels were 3.8 pmol/L (17.2 pg/mL) and morning cortisol was 115.8621 nmol/L (4.2 mcg/dL) (RV 5-25 mcg/dL or 140-690 nmol/L). Somatomedin C was measured at 85 ng/mL (RV 70-267 ng/mL) and prolactin at 3.5 ng/mL (RV 4-25 ng/mL). At the 1-year follow-up, the patient exhibited a satisfactory postoperative recovery. However, she developed diabetes insipidus and secondary hypothyroidism. Arterial hypertension persisted. Recent laboratory results indicated a glycated hemoglobin (HbA1c) level of 5.4%. Medications at the time of follow-up included prednisolone 5 milligrams a day, desmopressin 60 to 120 micrograms every 12 hours, losartan potassium 50 milligrams every 12 hours, and levothyroxine 88 micrograms a day.
Discussion
CD is associated with high mortality, primarily attributable to cardiovascular outcomes and comorbidities such as metabolic and skeletal disorders, infections, and psychiatric disorders [1]. The low incidence of CD in the context of the high prevalence of chronic noncommunicable diseases makes early diagnosis a challenge [2]. This case is relevant for reviewing the diagnostic approach process and highlighting the impact of the availability bias, which tends to prioritize more common diagnoses over rare diseases. Despite the absence of typical symptoms, a timely diagnosis was achieved.
Once exogenous CS is ruled out, laboratory testing must focus on detecting endogenous hypercortisolism to prevent misdiagnosis and inappropriate treatment [5]. Screening methods include 24-hour urinary free cortisol (UFC) for total cortisol load, while circadian rhythm and hypothalamic-pituitary-adrenal (HPA) axis function may be evaluated using midnight serum cortisol and LNSC [5]. An early hallmark of endogenous CS is the disruption of physiological circadian cortisol patterns, characterized by a constant cortisol level throughout the day or no significant decrease [2]. Measuring LNSC has proven to be useful in identifying these patients. The LNSC performed on the patient yielded a high result.
To assess HPA axis suppressibility, tests such as the overnight and the standard 2-day LDDST [5] use dexamethasone, a potent synthetic corticosteroid with high glucocorticoid receptor affinity and prolonged action, with minimal interference with cortisol measurement [6]. In a normal HPA axis, cortisol exerts negative feedback, inhibiting the secretion of corticotropin-releasing-hormone (CRH) and ACTH. Exogenous corticosteroids suppress CRH and ACTH secretion, resulting in decreased synthesis and secretion of cortisol. In pathological hypercortisolism, the HPA axis becomes partially or entirely resistant to feedback inhibition by exogenous steroids [5, 6]. The LDDST involves the administration of 0.5 mg of dexamethasone orally every 6 hours for 2 days, with a total dose of 4 mg. A blood sample is drawn 6 hours after the last administered dose [6]. Following the LDDST, the patient did not demonstrate suppression of endogenous corticosteroid production.
After diagnosing CS, the next step in the diagnostic pathway involves categorizing it as ACTH-independent vs ACTH-dependent. ACTH-independent cases exhibit low or undetectable ACTH levels, pointing to adrenal origin. The underlying principle is that excess ACTH production in CD can be partially or completely suppressed by high doses of dexamethasone, a response not observed in ectopic tumors [6]. In this case, the patient presented with an ACTH of 38.1 pg/mL (8.4 pmol/L), indicative of ACTH-dependent CD.
Traditionally, measuring cortisol levels and conducting pituitary imaging are standard practices for diagnosis. Recent advances propose alternative diagnostic methods such as positron emission tomography (PET) scans and corticotropin-releasing factor (CRF) tests [7]. PET scans, utilizing radioactive tracers, offer a view of metabolic activity in the adrenal glands and pituitary region, aiding in the identification of abnormalities associated with CD. Unfortunately, the availability of the aforementioned tests in the country is limited.
Once ACTH-dependent hypercortisolism is confirmed, identifying the source becomes crucial. A HDDST is instrumental in distinguishing between a pituitary and an ectopic source of ACTH overproduction [2, 6]. The HDDST involves administering 8 mg of dexamethasone either overnight or as a 2-day test. In this case, the patient received 2 mg of dexamethasone orally every 6 hours for 2 days, totaling a dose of 16 mg. Simultaneously, a urine sample for UFC is collected during dexamethasone administration. The HDDST suppressed endogenous cortisol production in the patient, suggesting a pituitary origin.
In ACTH-dependent hypercortisolism, CD is the predominant cause, followed by ectopic ACTH syndrome and, less frequently, an ectopic CRH-secreting tumor [3, 5]. With the pretest probability for pituitary origin exceeding 80%, the next diagnostic step is typically an MRI of the pituitary region. However, the visualization of microadenomas on MRI ranges from 50% to 70%, requiring further testing if results are negative or inconclusive [5]. Initial testing of our patient revealed no pituitary lesions. Following a pituitary location, ACTH-secreting tumors may be found in the lungs. Thus, a high-resolution chest computed tomography scan was performed, which yielded negative findings. Healthcare professionals must keep these detection rates in mind. In instances of high clinical suspicion, repeating or reassessing tests and imaging may be warranted [3], as in our case, ultimately leading to the discovery of a 4-mm pituitary adenoma.
It is fundamental to mention that the Endocrine Society Clinical Practice Guideline on Treatment of CS recommends that, when possible, all patients presenting with ACTH-dependent CS and lacking an evident causal neoplasm should be directed to an experienced center capable of conducting inferior petrosal sinus sampling to differentiate between pituitary and nonpituitary or ectopic cause [8]. However, in this instance, such a referral was regrettably hindered by logistical constraints.
Regarding patient outcomes and monitoring in CD, there is no consensus on defining remission criteria following tumor resection. Prolonged hypercortisolism results in suppression of corticotropes, resulting in low levels of ACTH and cortisol after surgical intervention. Typically, remission is identified by morning serum cortisol values below 5 µg/dL (138 nmol/L) or UFC levels between 28 and 56 nmol/d (10-20 µg/d) within 7 days after surgical intervention. In our case, the patient’s morning serum cortisol was 115.8621 nmol/L (4.2 µg/dL), indicating remission. Remission rates in adults are reported at 73% to 76% in selectively resected microadenomas and at 43% in macroadenomas [8], highlighting the need for regular follow-up visits to detect recurrence.
Following the surgery, the patient experienced diabetes insipidus, a relatively common postoperative occurrence, albeit usually transient [8]. It is recommended to monitor serum sodium levels during the first 5 to 14 days postsurgery for early detection and management. Additionally, pituitary deficiencies may manifest following surgery. In this patient, prolactin levels were compromised, potentially impacting sexual response. However, postoperative somatomedin levels were normal, and gonadotropins were not measured due to the patient’s age group, as no additional clinical decisions were anticipated based on those results. Secondary hypothyroidism was diagnosed postoperatively.
Moving forward, it is important to emphasize certain clinical signs and symptoms for diagnosing CD. The combination of low bone mineral density (Likelihood Ratio [LR] +21.33), central obesity (LR +3.10), and arterial hypertension (LR + 2.29) [9] has a higher positive LR than some symptoms considered “characteristic,” such as reddish-purple striae, plethora, proximal muscle weakness, and unexplained bruising [2, 10]. It is essential to give relevance to the signs the patient may present, emphasizing signs that have been proven to have an increased odds ratio (OR) such as osteoporosis (OR 3.8), myopathies (OR 6.0), metabolic syndrome (OR 2.7) and adrenal adenoma (OR 2.4) [9‐11]. The simultaneous development and worsening of these conditions should raise suspicion for underlying issues. Understanding the evolving nature of CD signs highlights the importance of vigilance during medical examinations, prioritizing the diagnostic focus, and enabling prompt initiation of treatment.
Recognizing the overlap of certain clinical features in CS is fundamental to achieving a timely diagnosis.
Learning Points
CS diagnosis is challenging due to the absence of pathognomonic signs and symptoms and the overlap of features present in many pathologies, such as metabolic syndrome.
Early detection of CS is crucial, given its association with high morbidity and mortality resulting from chronic exposure to glucocorticoids.
Recognizing the combination of low bone mineral density, obesity, hypertension, and diabetes as valuable clinical indicators is key in identifying CS.
Interdisciplinary collaboration is essential to achieve a comprehensive diagnostic approach.
Acknowledgments
We extend our gratitude to Pontificia Universidad Javeriana in Bogotá for providing essential resources and facilities that contributed to the successful completion of this case report. Special acknowledgment is reserved for the anonymous reviewers, whose insightful feedback significantly enhanced the quality of this manuscript during the peer-review process. Their contributions are sincerely appreciated.
Contributors
All authors made individual contributions to authorship. A.B.O. was involved in the diagnosis and management of this patient. M.A.G., J.M.H., and A.B.O. were involved in manuscript drafting and editing. All authors reviewed and approved the final draft.
Funding
This research received no public or commercial funding.
Disclosures
The authors declare that they have no conflicts of interest related to the current study.
Informed Patient Consent for Publication
Signed informed consent could not be obtained from the patient or a proxy but has been approved by the treating institution.
Data Availability Statement
Restrictions apply to the availability of some or all data generated or analyzed during this study to preserve patient confidentiality or because they were used under license. The corresponding author will on request detail the restrictions and any conditions under which access to some data may be provided.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted reuse, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Cushing’s disease (CD) is associated with a specific form of metabolic syndrome that includes visceral obesity, which may affect cardiovascular hemodynamics by stimulating hypercortisolism-related metabolic activity. The purpose of this study was to evaluate the relationship between obesity and the hemodynamic profile of patients with CD.
Methods: This prospective clinical study involved a hemodynamic status assessment of 54 patients newly diagnosed with CD with no significant comorbidities (mean age of 41 years). The assessments included impedance cardiography (ICG) to assess such parameters as stroke index (SI), cardiac index (CI), velocity index (VI), acceleration index (ACI), Heather index (HI), systemic vascular resistance index (SVRI), and total arterial compliance index (TACI) as well as applanation tonometry to assess such parameters as central pulse pressure (CPP) and augmentation index (AI). These assessments were complemented by echocardiography to assess cardiac structure and function.
Results: Compared with CD patients without obesity, individuals with CD and obesity (defined as a body mass index ≥ 30 kg/m2) exhibited significantly lower values of ICG parameters characterizing the pumping function of the heart (VI: 37.0 ± 9.5 vs. 47.2 ± 14.3 × 1*1000−1*s−1, p = 0.006; ACI: 58.7 ± 23.5 vs. 76.0 ± 23.5 × 1/100/s2, p = 0.005; HI: 11.1 ± 3.5 vs. 14.6 ± 5.5 × Ohm/s2, p = 0.01), whereas echocardiography in obese patients showed larger heart chamber sizes and a higher left ventricular mass index. No significant intergroup differences in blood pressure, heart rate, LVEF, GLS, TACI, CPP, or AI were noted.
Conclusions: Hemodynamic changes associated with obesity already occur at an early stage of CD and manifest via significantly lower values of the ICG parameters illustrating the heart’s function as a pump, despite the normal function of the left ventricle in echocardiography.
Cushing’s disease (CD), caused by a pituitary neuroendocrine tumor, leads to a specific type of metabolic syndrome that includes hypertension, obesity, impaired glucose metabolism, and dyslipidemia [1,2,3]. Chronic hypercortisolemia in patients with CD results in the excessive accumulation of visceral fat due to abnormal adipokine production [4]. Visceral obesity plays an important role in hypercortisolism-induced metabolic abnormalities and increased activity of the renin–angiotensin–aldosterone system activity in patients with CD [1,2,3,4,5]. Visceral obesity in patients with CD not only contributes to metabolic syndrome, but it is also an independent risk factor for cardiovascular disease [1,3,6,7]. Importantly, the structure and function of adipose tissue in patients with CD differ from those of healthy individuals [1,8,9]. The various hypercortisolism-induced metabolic abnormalities occurring in obese patients with CD may affect cardiovascular hemodynamics. There are no data on the effect of obesity on the hemodynamic profile of patients with CD and also few data are known on the association between obesity and hemodynamic disturbances in people without CD [10,11]. It was shown that the hemodynamic profile of a person with obesity is characterized by increased cardiac output and thoracic fluid content and decreased vascular resistance in comparison with these parameters in healthy individuals [12].
More studies are needed to enhance our understanding of the pathophysiology of CD-related obesity as a modifiable cardiovascular risk factor, in order to develop effective preventive and therapeutic strategies. Unfortunately, subclinical consequences of hypercortisolism in newly diagnosed patients with early CD, particularly with comorbid obesity, may be undetectable with standard methods. Therefore, novel and easy-to-use diagnostic methods would be of additive value to the standard methods of assessing cardiovascular structure and function in patients with CD. A detailed evaluation of the nature of obesity in patients with CD by innovative noninvasive diagnostic methods, such as impedance cardiography (ICG), applanation tonometry (AT), and echocardiographic assessment of global longitudinal strain (GLS), may provide additional data on cardiovascular hemodynamics, particularly the heart’s pumping function, preload, and afterload [13,14,15,16,17,18]. Our previous studies demonstrated the usefulness of ICG in identifying subclinical cardiovascular complications in patients with CD [19,20].
The purpose of this analysis was to assess the relationship between obesity and the hemodynamic profile of patients newly diagnosed with CD with no significant comorbidities.
2. Materials and Methods
2.1. Study Population
This was a prospective observational cohort study involving a comprehensive assessment of 54 patients (mean age of 41 years) newly diagnosed with CD with no significant comorbidities (although 64.8% were diagnosed with hypertension). These patients were admitted to the Military Institute of Medicine—National Research Institute between 2016 and 2021 in order to undergo a thorough cardiovascular assessment prior to transsphenoidal pituitary neuroendocrine tumor resection surgery.
This study was approved by the ethics committee at the Military Institute of Medicine—National Research Institute (approval No. 76/WIM/2016) and compliant with the Declaration of Helsinki and Good Clinical Practice guidelines. Each patient received detailed information on the purpose of this study and signed an informed consent form. This study was financed by the Polish Ministry of Research and Higher Education/Military Institute of Medicine—National Research Institute in Warsaw (grant No. 453/WIM).
2.2. Inclusion Criteria
The diagnosis of CD was established based on the presence of the typical (clinical and hormonal) evidence of hypercortisolism with no adrenocorticotropic hormone (ACTH) response to corticotropin-releasing hormone (CRH) stimulation, which meets the current guidelines for the diagnosis and treatment of CD [21,22,23]. Physical examination findings consistent with the signs and symptoms of CD, including central obesity with the characteristic altered body fat distribution (a moon face and a short, thick neck); muscle atrophy in the torso and limbs; purplish stretch marks on the abdomen, hips, and thighs; thinned skin; ecchymoses; signs and symptoms of hyperandrogenism; bone pain; frequent infections; erectile dysfunction in men; and secondary amenorrhea and infertility in women. Hormone test results included elevated 24 h urinary free cortisol levels, increased morning serum cortisol levels, altered circadian rhythmicity of ACTH and cortisol secretion, elevated or detectable morning serum ACTH, and a lack of overnight serum cortisol suppression to <1.8 mg/dL during a low-dose dexamethasone suppression test (1 mg or 2 mg of dexamethasone administered at midnight). In order to ensure a pituitary etiology of CD, all patients underwent a two-day high-dose (2 mg every 6 h = a total of 8 mg) dexamethasone suppression test (HDDST), which was expected to show low serum cortisol or a >50% decrease in urinary-free cortisol levels. Moreover, each patient was shown to have no ACTH secretion response to a CRH stimulation test (with 100 μg intravenous CRH), and the presence of a pituitary neuroendocrine tumor was confirmed via contrast magnetic resonance imaging of the pituitary. Patients with inconclusive hormone tests or imaging studies additionally underwent bilateral inferior petrosal sinus sampling (used to determine ACTH levels in the venous blood before and after CRH stimulation) [21,22,23].
2.3. Exclusion Criteria
The following comorbidities, which might considerably affect hemodynamic profiles, constituted our study exclusion criteria: (1) heart failure with mildly reduced or reduced left ventricular ejection fraction (LVEF) (i.e., LVEF of <50%); (2) cardiomyopathy; (3) clinically significant valvular heart disease or arrhythmia; (4) coronary artery disease, including a history of acute coronary syndrome; (5) a poor acoustic window on echocardiography; (6) a history of pulmonary embolism; (7) a history of a stroke or transient ischemic attack; (8) renal failure (estimated glomerular filtration rate < 60 mL/min/1.73 m2); (9) peripheral vascular disease and polyneuropathy; (10) chronic obstructive pulmonary disease; (11) respiratory failure (decreased partial pressure of arterial oxygen [PaO2] < 60 mmHg and/or increased partial pressure of carbon dioxide [PaCO2] > 45 mmHg); (12) a history of head trauma; (13) pregnancy; (14) age < 18 years; (15) no written informed consent.
2.4. Additional Hormone Tests
Due to the fact that hypercortisolemia inhibits gonadotropin release, hormone testing was expanded to include follicle-stimulating hormone and luteinizing hormone levels. The patients also had their serum thyroid-stimulating hormone levels tested to determine possible hypothyroidism, associated with reduced CRH and thyroid-stimulating hormone secretion and hypercortisolism-induced alterations in thyroid function. The patients with CD included in this study were not receiving any medications affecting the hypothalamus–pituitary–adrenal axis. None of the female patients with CD were pregnant at the time of the study or had given birth within the previous five years.
2.5. Laboratory Tests
In order to detect possible metabolic conditions, such as impaired fasting glucose, type 2 diabetes mellitus, or dyslipidemia, all patients underwent fasting blood tests from venous blood samples collected in the morning (at 6:00 a.m.). The tests evaluated the levels of fasting glucose, creatinine, eGFR, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglycerides, as well as a complete blood count.
2.6. Anamnesis and Physical Examination
The patients were thoroughly evaluated for cardiovascular risk factors, cardiovascular signs and symptoms, a family history of cardiovascular disease, comorbidities, prescription medications and other drugs, and smoking.
The body mass index (BMI) was calculated, and obesity was determined based on the International Diabetes Federation and European Society of Cardiology guidelines, which define it as a BMI of ≥30 kg/m2 [24,25]. In the study, patients were divided into two groups: patients with CD and obesity (defined as high body mass index ≥ 30 kg/m2) and patients with CD without obesity (defined as normal BMI < 30 kg/m2).
Physical examination included the resting heart rate (HR), systolic and diastolic blood pressure, and anthropometric parameters.
Office blood pressure measurements were taken by a trained nurse in seated patients in the morning, after a 5 min rest. The blood pressure monitor used was Omron M4 Plus (Omron Healthcare Co. Ltd., Kyoto, Japan), which meets the European Society of Cardiology criteria [26].
2.7. Echocardiography
Two-dimensional echocardiography included standard parasternal, apical, and subcostal views with a 2.5 MHz transducer (VIVID E95, GE Medical System, Wauwatosa, WI, USA) in accordance with the American Society of Echocardiography (ASE) and the European Association of Cardiovascular Imaging (EACVI) guidelines [27]. The parasternal long-axis view was used to measure the left ventricular end-diastolic diameter (LVEDd), right ventricular end-diastolic diameter (RVEDd), interventricular septal thickness, and left atrial (LA) diameter. Linear 2-dimensional left ventricular measurements were used to calculate the left ventricular mass index (LVMI), which is the left ventricular mass divided by the body surface area (LVMI cut-off values of >115 g/m2 for men and >95 g/m2 for women meet ASE and EACVI criteria for the diagnosis of left ventricular hypertrophy). The LVEF was calculated with the biplane Simpson method, based on 2-dimensional views of the left ventricle during systole and diastole in four- and two-chamber apical views. The ascending aortic diameter, valvular structure and function, and pericardium were assessed. The patients were assessed for left ventricular diastolic dysfunction according to current guidelines. Pulse wave Doppler in an apical four-chamber view aligned with mitral valve tips was used to visualize mitral inflow, including the early passive blood inflow (E) and the later atrial (A) contribution to the mitral inflow, E/A ratio, and early mitral inflow deceleration time. Apical four-chamber views were used to determine the septal and lateral early diastolic mitral annular velocities (e′ avg), and the E/e′ avg ratio was calculated [27,28].
Global longitudinal strain (GLS) was assessed via electrocardiography-gated automated function imaging in two-, three-, and four-chamber views. The rates of >60 frames per second were used for optimal speckle-tracking strain assessment. Patients with a poor acoustic window were excluded from the study. Semiautomated endocardial border detection was initiated by manually selecting two points identifying the mitral annulus and one point at the apex. Segmental and whole-chamber strain was assessed. The results have been presented in the form of a “bull’s eye” graph. The data were analyzed for four-, three-, and two-chamber views, and average GLS was calculated [29].
2.8. Impedance Cardiography
Based on the phenomenon of impedance variability in individual body segments associated with regional arterial blood flow, ICG is a noninvasive tool for assessing cardiovascular hemodynamics. ICG assessments were conducted by a trained nurse with a Niccomo device (Medis, Ilmenau, Germany) in patients who had been resting for 10 min in a supine position. ICG data were recorded during a 10 min assessment and processed with dedicated software (Niccomo Software, Medis). We analyzed the mean values of the following hemodynamic parameters reflecting the pumping function of the heart: (1) stroke volume (SV [mL]) and stroke index (SI [mL/m2]), based on the following formula: SV = VEPT × (dZmax/Z0) × LVET, where VEPT is tissue volume calculated from body weight, height, and patient sex, Z0 is the initial thoracic impedance, dZmax is the maximum change in thoracic impedance, and LVET is the left ventricular ejection time; (2) cardiac output (CO [mL] = SV × HR), and cardiac index (CI [mL*m−2*min−1]); (3) velocity index (VI [1*1000−1*s−1]); (4) acceleration index (ACI [1/100/s2], which is the peak acceleration of blood flow in the aorta; and (5) Heather index (HI [Ohm/s2] = dZmax × TRC, where TRC the time interval between the R-peak in the electrocardiogram and the C-point on the impedance wave). We also conducted a detailed analysis of the following afterload parameters: (1) systemic vascular resistance (SVR [dyn*s*cm−5]) together with SVR index (SVRI [dyn*s*cm−5*m2]) and (2) total arterial compliance (TAC) and TAC index (TACI [mL/mmHg] = SV/pulse pressure [mL/mmHg*m2]). Preload was assessed based on thoracic fluid content (TFC [1/kOhm], based on the formula TFC = 1000/Z0, where Z0 is the initial thoracic impedance [30,31,32].
2.9. Applanation Tonometry
Applanation tonometry is a novel method of indirectly illustrating arterial pressure waveform in the aorta and arterial stiffness, which reflect left ventricular afterload. AT parameters were assessed noninvasively with a SphygmoCor system (AtCor Medical, Sydney, NSW, Australia). The measurements were taken in supine patients by a qualified nurse immediately after ICG. Radial artery pressure curves were recorded via AT with a micromanometer (Millar Instruments, Houston, TX, USA) strapped onto the left wrist. We selected high-quality recordings for our analysis. Radial pulse was calibrated against the latest brachial systolic and diastolic blood pressure measurement with an oscillometric module of the Niccomo device. SphygmoCor software (version 9.0; AtCor Medical Inc. Pty Ltd., Sydney, NSW, Australia) was used to process the arterial waveform and generate an appropriate aortic blood pressure curve from the radial pulse curve. The analyzed waveforms were composed of the pulse wave generated by the aorta and were augmented by an overlapping reflected wave. Our analyses yielded the following parameters: central systolic blood pressure; central diastolic blood pressure; central pulse pressure (CPP); augmentation pressure, which is the absolute increase in aortic systolic pressure (directly generated by left ventricular contraction) resulting from the reflection wave; and the augmentation index, calculated as AP × 100/CPP, which is a quotient of the augmentation pressure and the blood pressure in the aorta [33].
2.10. Statistical Analysis
For the statistical analysis of the results, we used MS Office Excel 2023 and Statistica 12.0 (StatSof Inc., Tulsa, OK, USA). Data distribution and normality were assessed visually on histograms and with the use of the Kolmogorov–Smirnov test. Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR), and categorical variables were expressed as absolute and relative (percentage) values. In order to evaluate differences between the subgroups of CD patients with and without comorbid obesity, we used Student’s t-test for normally distributed data, and the Mann–Whitney U test for non-normally distributed data. A comparative analysis with the use of the Mann–Whitney U test was conducted on the data from patients stratified into two subgroups: patients with CD and obesity (BMI ≥ 30 kg/m2, n = 22) and patients with CD without obesity (BMI < 30 kg/m2, n = 32). The relationship between selected indices of cardiovascular function and obesity (represented as BMI) was analyzed separately for each one in a multivariable regression model, adjusting for age and hypertension as potential covariates related to hemodynamics. The threshold of statistical significance was adopted at p < 0.05.
3. Results
3.1. Baseline Characteristics
Nearly half of the patients with CD were found to be obese (n = 22, 40.7%). Overall, 20 of the 54 patients with Cushing’s disease (37%) were diagnosed with type 2 diabetes mellitus, 5 (9.3%) had prediabetes, and 29 (46.3%) had normal glucose tolerance. Of the patients with Cushing’s disease and type 2 diabetes, 14 received metformin, 5 received metformin with insulin, and 1 received insulin.
The mean age, HR, hemoglobin, creatinine, and sex distribution were similar in the subgroup with and without obesity (Table 1).
Table 1. Clinical, echocardiographic, hemodynamic, and applanation tonometry variables in patients with Cushing’s disease (CD) and with or without obesity.
3.2. Echocardiographic Assessment
Patients with CD and obesity (BMI ≥ 30 kg/m2) showed larger dimensions of heart chambers and ascending aorta (RVEDd, p < 0.001; LVEDd, p = 0.028; LA diameter, p < 0.001; aortic arch, p = 0.005) and higher rates of left ventricular mass index (LVMI, p = 0.028). We observed no significant differences between the subgroups in terms of the systolic (LVEF or GLS) or diastolic function of the left ventricle (Table 1).
3.3. ICG and AT Assessment
The most noticeable differences in ICG were observed for parameters of the left ventricular function as a pump. In obese individuals, VI (p = 0.006), ACI (p = 0.005), and HI (p = 0.012) were lower, whereas the systolic time ratio (STR) was higher (p = 0.038) than those in non-obese individuals, with SI and CI comparable in both subgroups. We observed no significant differences in afterload (TACI, SVRI, CPP, or augmentation index) or preload (TFC) parameters (Table 1).
3.4. Correlation Analysis
Analyzing the relationships between BMI and ICG hemodynamic parameters, we observed significant correlations, independent of sex and hypertension, between BMI and CI (R = 0.46; p < 0.001), SI (R = 0.29; p = 0.043), SVRI (−0.31; 0.028), and VI (R = −0.37; p = 0.0006)—see Table 2.
Table 2. Correlations between hemodynamic parameters assessed with impedance cardiography and body mass index, adjusted for sex and hypertension in multivariable regression models.
4. Discussion
The results of our study revealed a relationship between obesity and hemodynamic profile assessed via ICG in patients newly diagnosed with active CD. The use of novel diagnostic modalities demonstrated that excessive fat accumulation in young and middle-aged patients with CD, already at the early stages of the disease, is associated with some hemodynamic changes in the cardiovascular system, which—at that stage—may still be undetectable in routine assessments. These findings support the need for the early detection of subclinical heart dysfunction in patients with CD to enable early treatment and help prevent cardiovascular complications [1,34,35,36].
Occurring in 25%–100% of patients with CD, visceral obesity is one of the most common components of metabolic syndrome, often being the first sign of the disease. The duration of hypercortisolism correlates with obesity development [1,7,37,38], with chronic excessive cortisol levels being responsible for the abnormal distribution of adipose tissue [39]. The mechanisms behind this phenomenon may be due to the tissue overexpression of the 11β-hydroxysteroid dehydrogenase type 1 (11β-HSD1), which affects the pattern of excessive fat distribution in the torso, face, and neck [1,6]. Visceral obesity found in patients with CD is not only a component of metabolic syndrome but is in itself associated with increased metabolic activity, which makes it an independent cardiovascular risk factor, leading to the development of cardiovascular disease [1,4,9]. The tendency to accumulate visceral fat in patients with CD is also associated with abnormal adipokine production [4,6,40,41].
Our study included patients newly diagnosed with active CD with no clinically significant cardiovascular disease. Males were underrepresented in both subgroups. The proportion of patients with hypertension was 64.8%, which is comparable with that reported by other authors [38,42,43,44] and similarly distributed between subgroups. However, the patients in our study presented well-controlled hypertension (mean blood pressure was 126/83 mmHg), usually with one or two medications. Considering both sex and hypertension as potential confounders, these variables were included in regression models evaluating correlations between hemodynamics and BMI.
Similar to reports by other authors, our study showed higher SV and CO values in obese patients with CD; however, the respective indexed values (SI and CI) were comparable in obese and non-obese patients [12,45]. A more detailed ICG assessment demonstrated significant impairment of the pumping function of the heart as evidenced by lower HI, VI, and ACI values, and a higher STR value. The analysis of correlations revealed the independence of age and sex interrelation between some hemodynamic indices (CI, SI, SVRI, VI) and BMI. The paradox of the positive relation of obesity with volume indices of left ventricular function (CI and SI), which is negative with the marker of both its outflow and myocardial contractility (VI) encourages further studies investigating the (patho)physiological background of this phenomenon.
These findings were detected despite the lack of echocardiographic evidence of left ventricular systolic or diastolic dysfunction.
Moreover, our study showed larger heart chamber diameters and significantly higher LVMI in patients with CD and obesity, which is consistent with numerous earlier reports by other authors [46,47,48]. Nonetheless, it seems that in this case, increased heart chamber size and left ventricular hypertrophy should not be considered as only secondary to an increase in body weight. Hypercortisolism in patients with CD worsens the structural and functional condition of the heart muscle and may lead to myocardial fibrosis [48]. This results in myocardial remodeling associated with concentric left ventricular hypertrophy, which may impair left ventricular hemodynamic function, subsequently leading to myocardial dysfunction and symptomatic heart failure [49,50,51]. The effective treatment of patients with CD has been shown to normalize their serum cortisol levels and ultimately stop myocardial remodeling [47]. Therefore, the ICG-evidenced impaired pumping function of the heart may result from myocardial remodeling associated with complex metabolic and neuroendocrine changes in obese patients with CD [52]. These findings are consistent with previous reports on the adverse effect of obesity on left ventricular contractility [53,54,55,56].
The potential mechanisms underlying the results of our study remain to be elucidated. An interesting perspective is represented by the cross-talk between glucocorticoid (GR) and mineralocorticoid receptors (MR) and their impact on metabolic syndrome. Excessive activation of the MR in extra-renal tissues by aldosterone or glucocorticoids depending on the expression of 11beta-hydroxysteroid dehydrogenase type 2 has been shown to be associated with the development of vascular dysfunction and metabolic abnormalities, leading to obesity and metabolic syndrome. High concentrations of aldosterone may also activate the transcriptional function of the GR. These mechanisms result in an interaction between GR and MR in the regulation of adipogenesis [57].
The novelty of our approach is due to the use of noninvasive tools (ICG, AT) for hemodynamic assessment of the cardiovascular system in patients with CD to detect subclinical changes associated with obesity. On the one hand, our findings support earlier observations in other patient groups; on the other hand, they cast a new light on the relationship between obesity and an impaired hemodynamic profile in CD, which may result in the early development of cardiovascular complications.
4.1. Clinical Implications
We determined that a dysfunctional pumping action of the heart is the key marker of impaired cardiovascular hemodynamics in obese patients newly diagnosed with CD. The use of noninvasive diagnostic methods in this study revealed a complex relationship between obesity-related hemodynamic changes and the efficiency of left ventricular contractions. An early assessment of a patient’s hemodynamic profile may help detect subclinical cardiovascular dysfunction. Such a personalized approach may facilitate early therapeutic intervention and monitoring of treatment effectiveness focused on preventing myocardial remodeling and heart dysfunction.
4.2. Limitations
One limitation of our study was the small sample size. This was a result of the relatively low incidence of pituitary neuroendocrine tumors secreting ACTH. The exclusion of patients with clinically significant comorbidities further diminished the study population. However, this helped to eliminate the effect of additional factors on hemodynamic profiles. The patients assessed in our study were mostly young and middle-aged individuals with CD; therefore, our conclusions should not be extrapolated to older subjects. Although we conducted neither cardiac stress tests nor coronary angiography to exclude asymptomatic ischemic heart disease, other thorough assessments showed no physical, electrocardiographic, or echocardiographic evidence suggesting myocardial ischemia. Another potential limitation of our study is the fact that some patients had hypertension; however, it was well controlled with medications. The hemodynamic assessments involved the use of noninvasive methods as an alternative to the more expensive and less readily available invasive techniques. Nonetheless, we acknowledge the fact that noninvasive measurements can only provide indirect measurements and depend on the patient’s condition, which may vary over time.
5. Conclusions
The results of our study support the usefulness of ICG in diagnosing early heart dysfunction associated with obesity in patients with CD. Asymptomatic impairment of the heart’s pumping function seems to be the earliest clinical sign of cardiovascular hemodynamic abnormalities, which at this stage are still undetectable with standard echocardiography. Individual hemodynamic profile assessment with novel noninvasive diagnostic methods encourages further studies on cardiovascular system function in obese individuals with CD and on the use of personalized therapies, which aim at preventing adverse cardiovascular events.
Author Contributions
Conceptualization, A.J. and P.K.; methodology, A.J., P.K., G.G., B.U.-Ż., P.W. and G.Z.; software, P.K.; validation, A.J., P.K., B.U.-Ż., P.W. and G.Z.; formal analysis, P.K., P.W., G.G. and G.Z.; investigation, A.J., P.K., B.U.-Ż., P.W. and G.Z.; resources, A.J., P.K., B.U.-Ż., P.W. and G.Z.; data curation, A.J., P.K., B.U.-Ż., P.W., G.Z., A.K., R.W. and M.B.; writing—original draft preparation, A.J. and P.K.; writing—review and editing, G.G., B.U.-Ż., P.W. and G.Z.; visualization, A.J.; supervision, G.G. and G.Z.; project administration, G.Z.; funding acquisition, G.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Polish Ministry of Research and Higher Education/Military Institute of Medicine—National Research Institute in Warsaw (grant No. 453/WIM).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines and approved by the Bioethics Committee at the Military Institute of Medicine—National Research Institute in Warsaw, Poland (approval No. 76/WIM/2016; 21 December 2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
We would like to thank the medical personnel of the Military Institute of Medicine—National Research Institute in Warsaw for the provided patient care.
Conflicts of Interest
The authors declare no conflicts of interest.
References
Pivonello, R.; Isidori, A.M.; De Martino, M.C.; Newell-Price, J.; Biller, B.M.; Colao, A. Complications of Cushing’s syndrome: State of the art. Lancet Diabetes Endocrinol. 2016, 4, 611–629. [Google Scholar] [CrossRef]
Dekkers, O.M.; Horváth-Puhó, E.; Jørgensen, J.O.; Cannegieter, S.C.; Ehrenstein, V.; Vandenbroucke, J.P.; Pereira, A.M.; Sørensen, H.T. Multisystem morbidity and mortality in Cushing’s syndrome: A cohort study. J. Clin. Endocrinol. Metab. 2013, 98, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
Pivonello, R.; Faggiano, A.; Lombardi, G.; Colao, A. The metabolic syndrome and cardiovascular risk in Cushing’s syndrome. Endocrinol. Metab. Clin. N. Am. 2005, 34, 327–339. [Google Scholar] [CrossRef] [PubMed]
Pivonello, R.; De Leo, M.; Vitale, P.; Cozzolino, A.; Simeoli, C.; De Martino, M.C.; Lombardi, G.; Colao, A. Pathophysiology of diabetes mellitus in Cushing’s syndrome. Neuroendocrinology 2010, 1, 77–81. [Google Scholar] [CrossRef]
Davy, K.P.; Hall, J.E. Obesity and hypertension: Two epidemics or one? Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 286, R803–R813. [Google Scholar] [CrossRef]
Lee, M.J.; Pramyothin, P.; Karastergiou, K.; Fried, S.K. Deconstructing the roles of glucocorticoids in adipose tissue biology and the development of central obesity. Biochim. Biophys. Acta 2014, 1842, 473–481. [Google Scholar] [CrossRef] [PubMed]
Mancini, T.; Kola, B.; Mantero, F.; Boscaro, M.; Arnaldi, G. High cardiovascular risk in patients with Cushing’s syndrome according to 1999 WHO/ISH guidelines. Clin. Endocrinol. 2004, 61, 768–777. [Google Scholar] [CrossRef]
Bujalska, I.J.; Kumar, S.; Stewart, P.M. Does central obesity reflect “Cushing’s disease of the omentum”? Lancet 1997, 349, 1210–1213. [Google Scholar] [CrossRef]
Galton, D.J.; Wilson, J.P. Lipogenesis in adipose tissue of patients with obesity and Cushing’s disease. Clin. Sci. 1972, 43, 17P. [Google Scholar] [CrossRef]
Raison, J. Conséquences cardiovasculaires de l’obésité associée à l’hypertension artérielle [Cardiovascular consequences of obesity associated with arterial hypertension]. Presse Med. 1992, 21, 1522–1525. [Google Scholar]
de Simone, G.; Devereux, R.B.; Kizer, J.R.; Chinali, M.; Bella, J.N.; Oberman, A.; Kitzman, D.W.; Hopkins, P.N.; Rao, D.C.; Arnett, D.K. Body composition and fat distribution influence systemic hemodynamics in the absence of obesity: The HyperGEN Study. Am. J. Clin. Nutr. 2005, 81, 757–761. [Google Scholar] [CrossRef] [PubMed]
Krzesiński, P.; Gielerak, G.; Kowal, J. Kardiografia impedancyjna—Nowoczesne narzedzie terapii monitorowanej chorób układu krazenia [Impedance cardiography—A modern tool for monitoring therapy of cardiovascular diseases]. Kardiol. Pol. 2009, 67, 65–71. (In Polish) [Google Scholar]
El-Dawlatly, A.; Mansour, E.; Al-Shaer, A.A.; Al-Dohayan, A.; Samarkandi, A.; Abdulkarim, A.; Alshehri, H.; Faden, A. Impedance cardiography: Noninvasive assessment of hemodynamics and thoracic fluid content during bariatric surgery. Obes. Surg. 2005, 15, 655–658. [Google Scholar] [CrossRef] [PubMed]
Eikås, J.G.; Gerdts, E.; Halland, H.; Midtbø, H.; Cramariuc, D.; Kringeland, E. Arterial Stiffness in Overweight and Obesity: Association with Sex, Age, and Blood Pressure. High Blood Press Cardiovasc. Prev. 2023, 30, 435–443. [Google Scholar] [CrossRef] [PubMed]
Abomandour, H.G.; Elnagar, A.M.; Aboleineen, M.W.; Shehata, I.E. Subclinical Impairment of Left Ventricular Function assessed by Speckle Tracking in Type 2 Diabetic Obese and Non-Obese Patients: Case Control Study. J. Cardiovasc. Echogr. 2022, 32, 95–106. [Google Scholar] [CrossRef]
Galderisi, M.; Lomoriello, V.S.; Santoro, A.; Esposito, R.; Olibet, M.; Raia, R.; Di Minno, M.N.; Guerra, G.; Mele, D.; Lombardi, G. Differences of myocardial systolic deformation and correlates of diastolic function in competitive rowers and young hypertensives: A speckle-tracking echocardiography study. J. Am. Soc. Echocardiogr. 2010, 23, 1190–1198. [Google Scholar] [CrossRef]
Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
Jurek, A.; Krzesiński, P.; Gielerak, G.; Witek, P.; Zieliński, G.; Kazimierczak, A.; Wierzbowski, R.; Banak, M.; Uziębło-Życzkowska, B. Cushing’s Disease: Assessment of Early Cardiovascular Hemodynamic Dysfunction With Impedance Cardiography. Front. Endocrinol. 2021, 12, 751743. [Google Scholar] [CrossRef]
Jurek, A.; Krzesiński, P.; Uziębło-Życzkowska, B.; Witek, P.; Zieliński, G.; Kazimierczak, A.; Wierzbowski, R.; Banak, M.; Gielerak, G. The patient’s sex determines the hemodynamic profile in patients with Cushing disease. Front. Endocrinol. 2023, 14, 1270455. [Google Scholar] [CrossRef]
Fleseriu, M.; Auchus, R.; Bancos, I.; Ben-Shlomo, A.; Bertherat, J.; Biermasz, N.R.; Boguszewski, C.L.; Bronstein, M.D.; Buchfelder, M.; Carmichael, J.D.; et al. Consensus on diagnosis and management of Cushing’s disease: A guideline update. Lancet Diabetes Endocrinol. 2021, 9, 847–875. [Google Scholar] [CrossRef] [PubMed]
Nieman, L.K.; Biller, B.M.; Findling, J.W.; Newell-Price, J.; Savage, M.O.; Stewart, P.M.; Montori, V.M. The diagnosis of Cushing’s syndrome: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2008, 93, 1526–1540. [Google Scholar] [CrossRef]
Ceccato, F.; Boscaro, M. Cushing’s syndrome: Screening and diagnosis. High. Blood Press. Cardiovasc. Prev. 2016, 23, 209–215. [Google Scholar] [CrossRef]
Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef] [PubMed]
Bhalla, V.; Isakson, S.; Bhalla, M.A.; Lin, J.P.; Clopton, P.; Gardetto, N.; Maisel, A.S. Diagnostic Ability of B-Type Natriuretic Peptide and Impedance Cardiography: Testing to Identify Left Ventricular Dysfunction in Hypertensive Patients. Am. J. Hypertens. 2005, 18, 73S–81S. [Google Scholar] [CrossRef]
Parrott, C.W.; Burnham, K.M.; Quale, C.; Lewis, D.L. Comparison of Changes in Ejection Fraction to Changes in Impedance Cardiography Cardiac Index and Systolic Time Ratio. Congest. Heart Fail. 2004, 10, 11–13. [Google Scholar] [CrossRef]
Packer, M.; Abraham, W.T.; Mehra, M.R.; Yancy, C.W.; Lawless, C.E.; Mitchell, J.E.; Smart, F.W.; Bijou, R.; O’Connor, C.M.; Massie, B.M.; et al. Utility of Impedance Cardiography for the Identification of Short-Term Risk of Clinical Decompensation in Stable Patients with Chronic Heart Failure. J. Am. Coll. Cardiol. 2006, 47, 2245–2252. [Google Scholar] [CrossRef]
Pauca, A.L.; O’Rourke, M.F.; Kon, N.D. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension 2001, 38, 932–937. [Google Scholar] [CrossRef] [PubMed]
Coulden, A.; Hamblin, R.; Wass, J.; Karavitaki, N. Cardiovascular health and mortality in Cushing’s disease. Pituitary 2022, 25, 750–753. [Google Scholar] [CrossRef] [PubMed]
Clayton, R.N. Cardiovascular complications of Cushings syndrome: Impact on morbidity and mortality. J. Neuroendocrinol. 2022, 34, e13175. [Google Scholar] [CrossRef] [PubMed]
De Leo, M.; Pivonello, R.; Auriemma, R.S.; Cozzolino, A.; Vitale, P.; Simeoli, C.; De Martino, M.C.; Lombardi, G.; Colao, A. Cardiovascular disease in Cushing’s syndrome: Heart versus vasculature. Neuroendocrinology 2010, 1, 50–54. [Google Scholar] [CrossRef]
Faggiano, A.; Pivonello, R.; Spiezia, S.; De Martino, M.C.; Filippella, M.; Di Somma, C.; Lombardi, G.; Colao, A. Cardiovascular risk factors and common carotid artery caliber and stiff ness in patients with Cushing’s disease during active disease and 1 year after disease remission. J. Clin. Endocrinol. Metab. 2003, 88, 2527–2533. [Google Scholar] [CrossRef] [PubMed]
Witek, P.; Zieliński, G.; Szamotulska, K.; Witek, J.; Zgliczyński, W. Complications of Cushing’s disease—Prospective evaluation and clinical characteristics. Do they affect the efficacy of surgical treatment? Endokrynol. Pol. 2012, 63, 277–285. [Google Scholar] [PubMed]
Geer, E.B.; Shen, W.; Gallagher, D.; Punyanitya, M.; Looker, H.C.; Post, K.D.; Freda, P.U. MRI assessment of lean and adipose tissue distribution in female patients with Cushing’s disease. Clin. Endocrinol. 2010, 73, 469–475. [Google Scholar] [CrossRef] [PubMed]
Wang, M. The role of glucocorticoid action in the pathophysiology of the metabolic syndrome. Nutr. Metab. 2005, 2, 3. [Google Scholar] [CrossRef]
Tataranni, P.A.; Larson, D.E.; Snitker, S.; Young, J.B.; Flatt, J.P.; Ravussin, E. Eff ects of glucocorticoids on energy metabolism and food intake in humans. Am. J. Physiol. 1996, 271, E317–E325. [Google Scholar] [PubMed]
Isidori, A.M.; Graziadio, C.; Paragliola, R.M.; Cozzolino, A.; Ambrogio, A.G.; Colao, A.; Corsello, S.M.; Pivonello, R. ABC Study Group. The hypertension of Cushing’s syndrome: Controversies in the pathophysiology and focus on cardiovascular complications. J. Hypertens. 2015, 33, 44–60. [Google Scholar] [CrossRef]
Dekkers, O.M.; Biermasz, N.R.; Pereira, A.M.; Roelfsema, F.; van Aken, M.O.; Voormolen, J.H.; Romijn, J.A. Mortality in patients treated for Cushing’s disease is increased, compared with patients treated for nonfunctioning pituitary macroadenoma. J. Clin. Endocrinol. Metab. 2007, 92, 976–981. [Google Scholar] [CrossRef] [PubMed]
Lambert, J.K.; Goldberg, L.; Fayngold, S.; Kostadinov, J.; Post, K.D.; Geer, E.B. Predictors of mortality and long-term outcomes in treated Cushing’s disease: A study of 346 patients. J. Clin. Endocrinol. Metab. 2013, 98, 1022–1030. [Google Scholar] [CrossRef]
Abel, E.D.; Litwin, S.E.; Sweeney, G. Cardiac remodeling in obesity. Physiol. Rev. 2008, 88, 389–419. [Google Scholar] [CrossRef]
Hey, T.M.; Dahl, J.S.; Brix, T.H.; Søndergaard, E.V. Biventricular hypertrophy and heart failure as initial presentation of Cushing’s disease. BMJ Case Rep. 2013, bcr2013201307. [Google Scholar] [CrossRef] [PubMed]
Toja, P.M.; Branzi, G.; Ciambellotti, F.; Radaelli, P.; De Martin, M.; Lonati, L.M.; Scacchi, M.; Parati, G.; Cavagnini, F.; Cavagnini, F. Clinical relevance of cardiac structure and function abnormalities in patients with Cushing’s syndrome before and after cure. Clin. Endocrinol. 2012, 76, 332–338. [Google Scholar] [CrossRef]
You, K.H.; Marsan, N.A.; Delgado, V.; Biermasz, N.R.; Holman, E.R.; Smit, J.W.; Feelders, R.A.; Bax, J.J.; Pereira, A.M. Increased myocardial fibrosis and left ventricular dysfunction in Cushing’s syndrome. Eur. J. Endocrinol. 2012, 166, 27–34. [Google Scholar] [CrossRef]
Baykan, M.; Erem, C.; Gedikli, O.; Hacihasanoglu, A.; Erdogan, T.; Kocak, M.; Kaplan, S.; Kiriş, A.; Orem, C.; Celik, S. Assessment of left ventricular diastolic function and Tei index by tissue Doppler imaging in patients with Cushing’s Syndrome. Echocardiography 2008, 25, 182–190. [Google Scholar] [CrossRef]
Ainscough, J.F.; Drinkhill, M.J.; Sedo, A.; Turner, N.A.; Brooke, D.A.; Balmforth, A.J.; Ball, S.G. Angiotensin II type-1 receptor activation in the adult heart causes blood pressure-independent hypertrophy and cardiac dysfunction. Cardiovasc. Res. 2009, 81, 592–600. [Google Scholar] [CrossRef]
Uziębło-Życzkowska, B.; Krzesinński, P.; Witek, P.; Zielinński, G.; Jurek, A.; Gielerak, G.; Skrobowski, A. Cushing’s Disease: Subclinical Left Ventricular Systolic and Diastolic Dysfunction Revealed by Speckle Tracking Echocardiography and Tissue Doppler Imaging. Front. Endocrinol. 2017, 8, 222. [Google Scholar] [CrossRef]
Eschalier, R.; Rossignol, P.; Kearney-Schwartz, A.; Adamopoulos, C.; Karatzidou, K.; Fay, R.; Mandry, D.; Marie, P.Y.; Zannad, F. Features of cardiac remodeling, associated with blood pressure and fibrosis biomarkers, are frequent in subjects with abdominal obesity. Hypertension 2014, 63, 740–746. [Google Scholar] [CrossRef]
Krzesiński, P.; Stańczyk, A.; Piotrowicz, K.; Gielerak, G.; Uziębło-Zyczkowska, B.; Skrobowski, A. Abdominal obesity and hypertension: A double burden to the heart. Hypertens. Res. 2016, 39, 349–355. [Google Scholar] [CrossRef] [PubMed]
Wong, C.Y.; O’Moore-Sullivan, T.; Leano, R.; Byrne, N.; Beller, E.; Marwick, T.H. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation 2004, 110, 3081–3087. [Google Scholar] [CrossRef] [PubMed]
Parrinello, G.; Licata, A.; Colomba, D.; Di Chiara, T.; Argano, C.; Bologna, P.; Corrao, S.; Avellone, G.; Scaglione, R.; Licata, G. Left ventricular filling abnormalities and obesity-associated hypertension: Relationship with overproduction of circulating transforming growth factor beta1. J. Hum. Hypertens. 2005, 19, 543–550. [Google Scholar] [CrossRef] [PubMed]
Wang, Q.; Gao, Y.; Tan, K.; Li, P. Subclinical impairment of left ventricular function in diabetic patients with or without obesity: A study based on three-dimensional speckle tracking echocardiography. Herz 2014, 40, 260–268. [Google Scholar] [CrossRef]
Feraco, A.; Marzolla, V.; Scuteri, A.; Armani, A.; Caprio, M. Mineralocorticoid Receptors in Metabolic Syndrome: From Physiology to Disease. Trends Endocrinol. Metab. 2020, 31, 205–217. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.