Abstract
Objective
To investigate the outcomes of abnormal glucose metabolism and its clinical characteristics in patients with Cushing’s disease (CD) who achieved biochemical remission after surgery.
Methods
Patients diagnosed with CD who achieved biochemical remission and underwent regular follow-up after surgery were enrolled. Pre- and postoperative clinical data were collected and analyzed.
Result
151CD patients were included, of whom 80 (53 %) had preoperative abnormal glucose metabolism, including 56 with diabetes mellitus (DM) and 24 with impaired glucose regulation (IGR). At one year after surgery, 57 patients exhibited improved glucose metabolism, accompanied by a significant reduction in the homeostasis model assessment of insulin resistance (HOMA-IR). Improvements were mainly observed at 3 and 6 months after surgery. At one-year after surgery, there were 20 patients with diabetes and 16 with IGR. Compared to those with NGT, these individuals exhibited a higher prevalence of hypertension, hyperlipidemia, fatty liver, and abnormal bone metabolism.
Conclusion
CD patients demonstrated a high incidence of abnormal glucose metabolism. Notably, approximately two-thirds demonstrated improved glucose metabolism one year after curative surgery, with the greatest improvements observed at 3- to 6-month postoperative follow-up.
Introduction
Cushing’s disease (CD) is characterized by excessive endogenous cortisol production caused by pituitary adrenocorticotropic hormone adenoma and is the main cause of Cushing’s syndrome (CS). Surgical resection of the tumor is the preferred treatment. Prolonged exposure to hypercortisolism increases the risk of metabolic abnormalities, including obesity, hypertension, glucose and lipid abnormalities, osteoporosis, etc. Additionally, it significantly elevates the risk of infection, thrombosis, and hypokalemia. Abnormal glucose metabolism is a common complication of CS, with an incidence ranging from 13.1 % to 47 %[1], and diabetes is an independent risk factor for mortality in CD patients[2].
Previous clinical studies have found that metabolic abnormalities such as diabetes, hypertension, and hyperlipidemia improve in CS patients who achieve biochemical remission after surgical treatment. However, the concept of improvement in glucose metabolism, the incidence of improvement, and its related factors are inconsistent in various reports. Previous studies primarily assessed the outcome of glucose metabolism based on plasma glucose results at a single fixed follow-up time after surgery. The lack of regular follow-up data makes it difficult to clearly understand the trend of postoperative plasma glucose changes, and there are no clinical data on when glucose metabolism begins to improve or change. Therefore, this study retrospectively analyzed the follow-up data of patients with Cushing’s disease in our hospital before and after surgery, and monitored the changes in glucose metabolism, to explore the characteristics and clinical features of such changes in patients with Cushing’s disease who achieved remission from CD following surgery..
Access through your organization
Check access to the full text by signing in through your organization.
Section snippets
Subjects
This study enrolled hospitalized patients with Cushing’s disease at Huashan Hospital, Fudan University from January 2014 to February 2020. Inclusion criteria were as follows: (1) Age ≥ 18 years; (2) diagnosis of Cushing’s disease according to the 2021 Consensus on the Diagnosis and Management of Cushing’s Disease, confirmed by pathology[3]; (3) biochemical remission after transsphenoidal surgery; (4) complete preoperative data and regular follow-up visits (including visits at 1, 3, 6, and
Patients’ baseline characteristics
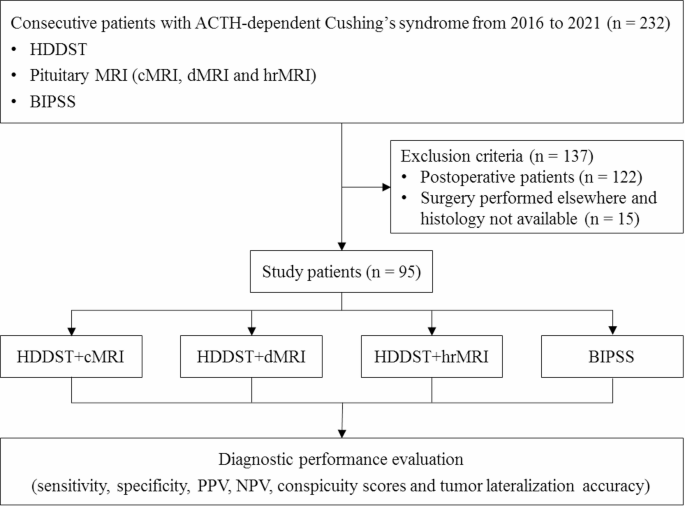
A total of 168 patients with CD were admitted to Huashan Hospital from 2014 to 2020 with pathological diagnosis and regular postoperative follow-up; however, 17 patients were excluded due to no biochemical remission after surgery or relapse during follow-up (Fig. 1). Ultimately, 151 patients (32 males and 119 females) were included in this study. The baseline characteristics of the included patients were shown in Table 1. There were 80 cases (53 %) complicated with abnormal glucose metabolism
Discussion
CD was a rare disease often associated with abnormal glucose metabolism. Based on medical history and OGTT screening, we found that over half (53 %) of CD patients exhibited abnormal glucose metabolism before surgery, with 37.1 % being diagnosed with diabetes. Previous studies have shown that the prevalence of diabetes in CS patients ranged from 13.1 % to 47 %, and most reports falling between 35 % and 45 %, which is consistent with our findings [1,12,13]. However, it should be noted that CD
Author contributions
Q.C. analyzed the data and wrote the manuscript. Q.C., Y.L., X.L., Q.S., W.S., and H.Z. collected the data. Y.L., Z.Z., M.H., S.Z., and H.Y. recruited patients. J.Z., Y.S., and S.Z. conducted the study design and revised the manuscript. All authors read and approved the final manuscript.
CRediT authorship contribution statement
Qiaoli Cui: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Yujia Li: Writing – original draft, Investigation, Formal analysis, Data curation. Xiaoyu Liu: Investigation, Formal analysis, Data curation. Quanya Sun: Investigation, Data curation. Wanwan Sun: Investigation, Formal analysis, Data curation. Min He: Project administration, Investigation. Jie Zhang: Writing – review & editing, Supervision, Funding
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments
We are indebted to the patients who participated in this study and all the doctors who contributed to the diagnosis and treatment of these patients. This work was supported by grants from the Multidisciplinary Diagnosis and Treatment (MDT) demonstration project in research hospitals (Shanghai Medical College, Fudan University, NO: DGF501069/017), National Science and Technology Major Project (NO: 2023ZD0506800,2023ZD0506802), 2023 Ningbo International Cooperation Program (NO: 2023H024).
References (16)
- R.N. Clayton et al.
Mortality in patients with Cushing’s disease more than 10 years after remission: a multicentre, multinational, retrospective cohort study
Lancet Diabetes Endocrinol
(2016) - M. Fleseriu et al.
Consensus on diagnosis and management of Cushing’s disease: a guideline update
Lancet Diabetes Endocrinol
(2021) - C. Scaroni et al.
Glucose Metabolism Abnormalities in Cushing Syndrome: from Molecular Basis to Clinical Management
Endocr Rev
(2017) - C. Dai et al.
Surgical outcome of transsphenoidal surgery in Cushing’s disease: a case series of 1106 patients from a single center over 30 years
Endocrine
(2022) - E. Valassi et al.
Delayed remission after transsphenoidal surgery in patients with Cushing’s disease
J Clin Endocrinol Metab
(2010) - X. He et al.
Glucocorticoid Withdrawal Syndrome following treatment of endogenous Cushing Syndrome
(2022) - E.V. Varlamov et al.
Perioperative Management of a Patient with Cushing Disease
J Endocr Soc
(2022) - Q. Cui et al.
The recovery time of hypothalamic-pituitary-adrenal axis after curative surgery in Cushing’s disease and its related factor
Endocrine
(2023)
There are more references available in the full text version of this article.
Filed under: Cushing's, pituitary, Treatments | Tagged: diabetes mellitus, glucose, pituitary, post-op, remission, surgery | Leave a comment »