Neuroendocrine neoplasms (NENs) causing ectopic Cushing’s syndrome (ECS) are rare and challenging to treat. In this retrospective cohort study, we aimed to evaluate different approaches for bilateral adrenalectomy (BA) as a treatment option in ECS. Fifty-three patients with ECS caused by a NEN (35 females/18 men; mean ± SD age: 53 ± 15 years) were identified from medical records. Epidemiological and clinical parameters, survival, indications for surgery and timing, as well as duration of surgery, complications and surgical techniques, were collected and further analysed. The primary tumour location was thorax (n = 30), pancreas (n = 14) or unknown (n = 9). BA was performed in 37 patients. Median time from diagnosis of ECS to BA was 2 months (range 1–10 months). Thirty-two patients received different steroidogenesis inhibitors before BA to control hypercortisolaemia. ECS resolved completely after surgery in 33 patients and severe peri- or postoperative complications were detected in 12 patients. There were fewer severe complications in the endoscopic group compared to open surgery (p = .030). Posterior retroperitoneoscopic BA performed simultaneously by a two surgeon approach had the shortest operating time (p = .001). Despite the frequent use of adrenolytic treatment, BA was necessary in a majority of patients to gain control over ECS. Complication rate was high, probably as a result of the combination of metastatic disease and metabolic disorders caused by high cortisol levels. The two surgeon approach BA may be considered as the method of choice in ECS compared to other BA approaches as a result of fewer complications and a shorter operating time.
1 INTRODUCTION
Endogenous Cushing’s syndrome (CS) has an estimated incidence of 0.2–5.0 per million people per year.1 In 5–10% of these, it is caused by ectopic secretion of adrenocorticotrophic hormone (ACTH) or, in extremely rare cases, corticotrophin-releasing hormone, from a non-pituitary tumour.1, 2
The treatment of neuroendocrine neoplasms (NENs) with ectopic secretion of ACTH is challenging. Because of the rarity and heterogeneity of this condition, there is no established evidence-based recommendation.3 Most patients with ectopic Cushing’s syndrome (ECS) have severe hypercortisolaemia leading to disrupted electrolyte and glucose levels, metabolic alkalosis, thrombosis and life-threatening infections, amongst many other manifestations. Initiation of oncological treatment is often delayed as a result of the consequences of high cortisol levels. A reduction of the cortisol level is crucial for survival and hypercortisolaemia and hypokalaemia are negative prognostic factors.4, 5 If radical surgery of the tumour is not possible because of metastatic disease, normo-cortisolaemia can be achieved either by medical treatment with steroidogenesis inhibitors (SI) or bilateral adrenalectomy (BA),6 and BA has also been considered a treatment option for patients with occult or cyclic ECS. In patients with metastatic neuroendocrine carcinomas, platinum-based chemotherapy may be applied as first-line action, combined by SI and/or followed by BA. Computed tomography-guided percutaneous adrenal ablation has been reported in several case reports as a possible therapeutic alternative for patients in whom medical treatment has failed and BA is not feasible,7–10 althhough more data is needed to recommend this method in daily practice.
In the 1930s, transabdominal open access BA was introduced as a treatment option for uncontrolled cortisol secretion.11 Sixty years later, in the 1990s, laparoscopic methods were established12, 13 and are now considered as the gold standard for BA (except for adrenal carcinomas) because they result in less postoperative pain, a shorter hospitalisation time and faster recovery.14 Laparoscopic transperitoneal adrenalectomy (LTA) is the most frequently applied surgical method. However, posterior retroperitoneoscopic adrenalectomy (PRA), introduced in 1995 by Walz et al,15 is gaining popularity.16 Using PRA compared to LTA offers a more direct approach to the adrenal glands, a shorter operating time (no need for reposition of the patient), less blood loss and faster recovery, and it aso has advantages for patients with obesity or a history of previous abdominal surgery.16 There are centres where PRA is performed by a two surgeon approach; thus, a simultaneous bilateral approach offers the possibility of decreasing the surgical time by up to 50% and reducing operative stress.17–19
The present study aimed to evaluate BA as a treatment option for ECS, as well as the effects of different approaches on morbidity and mortality. We hypothesised that endoscopic surgery methods could be superior regarding complication rate, operating and hospitalisation time compared to open access surgery and also influence overall survival.
2 MATERIALS AND METHODS
2.1 Patients and data
A cohort of 59 patients with ECS was identified retrospectively from medical records of 894 patients with NENs, referred to the Department of Endocrine Oncology, Uppsala University Hospital between 1984 and 2019. None of the patients had a small-cell lung cancer (SCLC) because these tumours are not treated at our centre and possibly have a different mechanism behind ACTH production compared to that of NENs. Furthermore, SCLCs have a much more severe course of disease compared to well differentiated NENs and including them in the present study could mask any results important for NEN clinical management. Six patients were from outside Sweden and were excluded from further analysis because of a lack of follow-up data; thus, in total, 53 patients were available for analysis. Diagnosis of ECS was confirmed by histopathological examination of tumour specimen (n = 48) together with the clinical and biochemical picture of ACTH-dependent Cushing’s syndrome (elevated serum and urinary cortisol, high ACTH and pathological functional tests). In five patients where neither primary tumor, nor metastatic disease was found despite several PET examinations, including 68 Ga- DOTATOC-PET, 11C-5HTP-PET and 18FDG-PET in four of the five patients, ECS was confirmed on the basis of the clinical/biochemical picture and exclusion of pituitary origin by magnetic resonance imaging, as well as inferior sinus petrosus sampling.
Epidemiological data, data on clinical parameters, survival, indication and duration of surgery, complications and surgical technique were extracted and further analysed.
2.2 Surgery
BA was performed either by an open access approach, LTA or PRA. PRA was performed either by one surgeon (PRA-1S) or by two surgeons operating on both sides simultaneously (PRA-2S). Some patients were operated twice (one adrenal at the time) and, for those patients, operating time was pooled from both surgeries, if both sessions were performed within 1 week. Cases where conversion from an endoscopic to an open access approach was made peroperatively were grouped as open access surgery in further analysis. Patients who died during the postoperative stage (within 30 days) were excluded from calculation of hospitalisation time.
Postoperative complications were graded using the Clavien–Dindo classification where complications of Grade 1 are defined as “any deviation from the normal postoperative course without the need for pharmacological treatment or surgical, endoscopic and radiological interventions. Allowed therapeutic regimens are drugs as antiemetics, antipyretics, analgesics, diuretics and electrolytes and physiotherapy”.20 Because almost all patients had mild, Grade 1 postoperative complications (metabolic disturbances caused by hypercortisolaemia), this variable is not described. We defined complications up to Grade 2 as mild and Grade 3–5 as severe.
2.3 Statistical analysis
All parameters were analysed by descriptive statistics: normally distributed data as the mean ± SD, and data with skewed distribution and/or outliers were described as medians, accompanied by the 25th to 75th percentile ranges (Q1-Q3) or minimum-maximum (min-max). The defined event was death from any cause. Overall survival (OS) was defined as time from diagnosis of ECS or time of BA until date of death or, if the event was not found, censored at date of last observation, 31 December 2019. Kaplan-Meier plots were used for survival analysis and the log-rank test was used for comparison. Chi-squared was used for testing relationships between categorical variables. p < .05 was considered statistically significant. All statistical analyses were performed using IBM, version 27 (IBM Corp., Armonk, USA).
3 RESULTS
3.1 Studied patients
ECS represented six% (n = 59) of NENs in our cohort. Six patients were excluded from further analysis, resulting in 53 ECS patients who were analysed; there were 35 females and 18 males with a mean ± SD age of 53 ± 15 years. The localisation of the primary NEN was thorax (n = 30), pancreas (n = 14) or unknown (n = 9). Histopathological staining for Ki-67 was available in 38 patients and Ki-67 was < 2% in five patients, 3–20% in 22 patients and > 20% in 11 patients. Patient characteristics are shown in Tables 1 and 2. Twenty-two patients (41.5%) in this cohort had concomitant hypersecretion of hormones other than ACTH from their tumour (5-HIAA, n = 10; calcitonin, n = 3; 5-HIAA + calcitonin, n = 2; glucagon, n = 3, gastrin, n = 2; growth hormone, n = 1; insulin + gastrin + vasointestinal peptide, n = 1).
3.2 Surgery
Adrenalectomy was performed in 37 patients (70%); 24 patients were operated at Uppsala University Hospital, nine at Karolinska University Hospital in Stockholm and four at Umeå University Hospital. Median time from diagnosis of ECS to BA was 2 months (range 1–10 months). Median Ki-67 in patients who were operated within 2 months after ECS diagnosis was higher (Ki-67 18.5%) compared to those with BA performed later in the course of disease (Ki-67 9.5%), although the difference was not statistically significant (p = .085).
Thirty-two (86%) patients received different SI prior to BA to control hypercortisolaemia. Eight of those were treated with chemotherapy as well in an attempt to reduce cortisol levels. The majority of patients was treated with ketoconazole, often in combination with other drugs (Table 3). Indications for BA in our cohort included (1) persistent hypercortisolaemia despite use of SI (n = 30); (2) BA as first choice of treatment to reduce cortisol levels (n = 5); and (3) no effect combined with severe side effects from SI including liver toxicity and severe leukopenia (n = 2). In 16 patients, BA was not performed as a result of (1) good control of ECS with SI (n = 4); (2) radical surgery of the primary tumour (n = 3); (3) good control of ECS with SI followed by radical surgery of the primary tumour (n = 5) and (4) the bad condition of the patient (n = 4).
3.3 Survival analysis
There was no operative mortality in this cohort. Four patients died within 1 month after adrenalectomy (on day 5, 16, 22 and 30, respectively) as a result of multiple organ dysfunction syndrome and progression of NEN. At the end of the follow-up period, 14 patients were still alive and 39 had died.
Median survival after BA was 24 months (95% confidence interval [CI] = 7–41, min-max: 0–428) with a 5-year survival of 22%. Median follow-up time for all patients from time of ECS diagnosis was 26 (range 6–62) months and after BA was 19 (range 3–50) months. OS was longer in patients where ECS was treated by radical surgery of the primary tumour or where good biochemical control was achieved by SI compared to patients who underwent BA, 96 months (95% CI 0–206) vs 29 months (95% CI 7–51), respectively. However, this difference was not statistically significant (p = .086), most likely as a result of the small sample size. Multiple hormone secretion correlated with shorter OS after BA (p = .009; hazard ratio = 2.9; 95% CI= 1.3–6.7). There was no significant difference in OS after BA depending on localisation of primary tumour (thoracic NENs 24 months [95% CI = 8–40, min-max: 0–428], pancreatic NENs 19 months [95% CI = 0–43, min-max: 0–60], p = .319) or surgical approach (open access approach 24 months [95% CI = 1–47], endoscopic approach 19 months [95% CI = 1–37], p = .720).
Median time from ECS diagnosis to BA was 2 months (range 1–10). Patients who underwent BA within 2 months after ECS diagnosis had shorter OS compared to those who were operated at a later stage: 6 months (95% CI = 0–18) and 45 months (95% CI = 3–86) respectively (p = .007). The former group had a slightly higher median Ki-67 level (18% vs 9%), lower potassium (2.7 mmol L-1 vs 3.0 mmol L-1) and higher hormone levels (ACTH 217 vs 120 ng mL-1, morning cortisol 1448 vs 1181 nmol L-1 and UFC 5716 vs 4234 nmol per 24 h) at diagnosis compared to those who were operated later in the course of disease.
4 DISCUSSION
The present study highlights new aspects of the advantages of an endoscopic approach of BA compared to open access surgery, regarding the incidence of severe complications graded using the Clavien-Dindo classification, as well as operation- and hospitalisation time. Our results indicate that PRA performed by two surgeons simultaneously is the method of choice for patients with ECS. However, despite these advantages, the endoscopic approach did not appear to improve overall survival.
Recent Endocrine Society guidelines recommend SI as primary treatment for ECS in patients with occult or metastatic ECS followed by BA.6 Although the toxicity of SI in our cohort was low (n = 2; 6%), 32 patients (73%) had persistent hypercortisolaemia despite medical treatment and proceeded to BA. BA, especially with an endoscopic approach, with a short operating time and low complication risk, appears to play a major role in the appropriate management of hypercortisolaemia in ECS, where rapid reduction of cortisol levels is very important.
Prolonged exposure to high cortisol levels, in combination with high risk for hepatotoxic and nephrotoxic SI side effects, increases morbidity and risk for severe complications, and often delays the start of oncological treatment. However, the trauma caused by surgery can also postpone initiation of chemotherapy.21 Therefore, a fast and minimally invasive surgical procedure appears to be a crucial factor for the better survival in ECS. The endoscopic approach is now considered as the gold standard for BA. Our study presents fewer severe complications, as well as shorter operating and hospitalisation times, when the endoscopic approach is compared with open surgery. In line with previous studies,19, 22 we observed a significantly shorter operating time when applying PRA compared to LTA because there is no need for repositioning of the patient during PRA. PRA-2S had the shortest operating time and should be considered as the best choice of surgical approach in ECS. This result ties well with previous studies reporting the median operating time to be between 43 and 157 min in PRA-2S, which is significantly shorter compared to LTA and PRA-1S.17–19
The median time from diagnosis to BA was 2 months, which is consistent with a previous study.23 However, OS was significantly shorter in patients who were operated within 2 months after diagnosis of ECS in our cohort compared to those operated at a later stage. These early operated patients probably had a more aggressive clinical course of disease, as indicated by slightly higher median Ki-67, lower potassium and higher hormone levels at diagnosis, and they were operated as a result of more acute indications (without time to proper pre-treatment with SI) than the other group.
In our previous report on patients with ACTH-producing NENs, multiple hormone secretion was identified as the strongest indicator of a worse prognosis.4 A similar pattern of results was observed in this cohort, showing that patients with NENs, with concomitant hypersecretion of other hormones than ACTH from their tumour, had a shorter OS after BA compared to those with ACTH hypersecretion only.
As a result of the extremely high preoperative cortisol levels in ECS, the substitution therapy needed after successful BA may be challenging.21 Over-replacement of glucocorticoids may lead to higher morbidity24 and mortality, especially in patients with metastatic NENs, who often have impaired immune function because of oncological treatment. Many patients suffer from glucocorticoid withdrawal syndrome, despite adequate replacement therapy, and it can take ≥ 1 year to gain control over these symptoms.6 This frequently leads to high dosage of glucocorticoids. The Endocrine Society guidelines recommend glucocorticoid replacement with hydrocortisone, 10–12 mg m-2 day-1 in divided doses.6 If we assume that most of our patients have body surface area around 2 m2 or less, the daily hydrocortisone dose should not exceed 25 mg. However, 1 year after BA, only one patient received 25 mg of hydrocortisone daily, with the majority receiving 30 mg or more. One-third of the patients had residual arterial hypertension and diabetes 3 months after BA, probably partially depending on too high a dose of glucocorticoids.
There was a higher complication rate in our cohort compared to other studies19, 25, 26 and five patients needed conversion from an endoscopic approach to open surgery. In particular, the outcome of BA in ECS has not previously been systematically evaluated27 because most of the reports include patients with various aetiologies of CS.19, 22, 23, 28, 29 In a systematic review of the literature published between 1980 and 2012 on BA in CS, Reincke et al23 identified 37 studies and ECS was present in 13% of the patients. There are only few papers focused on BA in ECS solely21, 25, 26, 30, 31 and only one has a cohort with > 50 patients (n = 54).26 Patients with ECS have almost always a more aggressive course and more severe metabolic disturbance than patients with other types of Cushing’s syndrome, which probably leads to higher risk for postoperative complications. Furthermore, multiple liver metastases, fibrotic processes in the abdomen as a result of previous surgery or large primary tumour in pancreas could be some of the factors influencing surgical outcome in ECS.
The present study has several limitations. First, all data were collected retrospectively from patient records and not all the preferred parameters were available for all patients. Second, even if our cohort is one of the largest regarding studies on BA in ECS, the number of patients is too low for reliable statistical analysis. Finally, our study covered more than three decades, BAs were performed at different clinics and by different surgeons. Therefore, the data should be interpreted carefully.
In conclusion, the present study is one of few reports focusing on BA in specifically NEN patients with ECS and includes one of the largest patient cohorts analysed in the field. PRA-2S can be considered as method of choice in ECS compared to other BA approaches. The aim is to avoid administrating too high a hydrocortisone replacement dosage postoperatively because this can worsen the metabolic disturbance. As a result of the rarity of the condition, multicentre studies are needed with large, prospective cohorts and standardised inclusion criteria, aiming to further improve our knowledge about the management of ECS.
ACKNOWLEDGEMENTS
This study was funded by the Swedish Cancer Society (grant number CAN 18 0576), the Lions Foundation for Cancer Research at Uppsala University Hospital, Selanders Foundation and Söderbergs foundation at Uppsala University.
CONFLICT OF INTERESTS
The authors declare that they have no conflicts of interest.
The need for informed consent was waived by the local ethics committee. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the local ethics committee, Regionala etikprövningsnämnden (EPN), in Uppsala, Sweden.
Cushing disease is caused by tumour in the pituitary gland which leads to excessive secretion of a hormone called adrenocorticotrophic (ACTH), which in turn leads to increasing levels of cortisol in the body. Cortisol is a steroid hormone released by the adrenal glands and helps the body to deal with injury or infection.
Increasing levels of cortisol increases the blood sugar and can even cause diabetes mellitus. However the disease is also caused due to excess production of hypothalamus corticotropin releasing hormone (CRH) which stimulates the synthesis of cortisol by the adrenal glands. The condition is named after Harvey Cushing, the doctor who first identified the disease in 1912. Cushing disease results in Cushing syndrome.
Cushing syndrome is a group of signs and symptoms developed due to prolonged exposure to cortisol. Signs and symptoms of Cushing syndrome includes hypertension, abdominal obesity, muscle weakness, headache, fragile skin, acne, thin arms and legs, red stretch marks on stomach, fluid retention or swelling, excess body and facial hair, weight gain, acne, buffalo hump, tiredness, fatigue, brittle bones, low back pain, moon shaped face etc. Symptoms vary from individual to individual depending upon the disease duration, age and gender of the patient.
Disease diagnosis is done by measuring levels of cortisol in patient’s urine, saliva or blood. For confirming the diagnosis, a blood test for ACTH is performed. The first-line treatment of the disease is through surgical resection of ACTH-secreting pituitary adenoma, however disease management is also done through medications, Cushing disease treatment market comprises of the drugs designed for lowering the level of cortisol in the body. Thus patients suffering from Cushing disease are prescribed medications such as ketoconazole, mitotane, aminoglutethimide metyrapone, mifepristone, etomidate and pasireotide.
Cushing’s disease treatment market revenue is growing with a stable growth rate, this is attributed to increasing number of pipeline drugs. Also increasing interest of pharmaceutical companies to develop Cushing disease drugs is a major factor contributing to the revenue growth of Cushing disease treatment market over the forecast period.
Current and emerging players’ focuses on physician education and awareness regarding availability of different drugs for curing Cushing disease, thus increasing the referral speeds, time to diagnosis and volume of diagnosed Cushing disease individuals.
Growing healthcare expenditure and increasing awareness regarding Cushing syndrome aids in the revenue growth of Cushing’s disease treatment market. Increasing number of new product launches also drives the market for Cushing’s disease Treatment devices. However availability of alternative therapies for curing Cushing syndrome is expected to hamper the growth of the Cushing’s disease treatment market over the forecast period.
The Cushing’s disease Treatment market is segment based on the product type, technology type and end user
Cushing’s disease Treatment market is segmented into following types:
By Drug Type
Ketoconazole
Mitotane
Aminoglutethimide
Metyrapone
Mifepristone
Etomidate
Pasireotide
By End User
Hospital Pharmacies
Retail Pharmacies
Drug Stores
Clinics
e-Commerce/Online Pharmacies
Cushing’s disease treatment market revenue is expected to grow at a good growth rate, over the forecast period. The market is anticipated to perform well in the near future due to increasing awareness regarding the condition. Also the market is anticipated to grow with a fastest CAGR over the forecast period, attributed to increasing investment in R&D and increasing number of new product launches which is estimated to drive the revenue growth of Cushing’s disease treatment market over the forecast period.
Depending on geographic region, the Cushing’s disease treatment market is segmented into five key regions: North America, Latin America, Europe, Asia Pacific (APAC) and Middle East & Africa (MEA).
North America is occupying the largest regional market share in the global Cushing’s disease treatment market owing to the presence of more number of market players, high awareness levels regarding Cushing syndrome. Healthcare expenditure and relatively larger number of R&D exercises pertaining to drug manufacturing and marketing activities in the region. Also Europe is expected to perform well in the near future due to increasing prevalence of the condition in the region.
Asia Pacific is expected to grow at the fastest CAGR because of increase in the number of people showing the symptoms of Cushing syndrome, thus boosting the market growth of Cushing’s disease treatment market throughout the forecast period.
Some players of Cushing’s disease Treatment market includes CORCEPT THERAPEUTICS, HRA Pharma, Strongbridge Biopharma plc, Novartis AG, etc. However there are numerous companies producing branded generics for Cushing disease. The companies in Cushing’s disease treatment market are increasingly engaged in strategic partnerships, collaborations and promotional activities to capture a greater pie of market share.
The research report presents a comprehensive assessment of the market and contains thoughtful insights, facts, historical data, and statistically supported and industry-validated market data. It also contains projections using a suitable set of assumptions and methodologies. The research report provides analysis and information according to categories such as market segments, geographies, types, technology and applications.
Bilateral adrenalectomy (BA) still plays an important role in the management of Cushing’s disease (CD). Nelson’s syndrome (NS) is a severe complication of BA, but conflicting data on its prevalence and predicting factors have been reported. The aim of this study was to determine the prevalence of NS, and identify factors associated with its development.
Data sources
Systematic literature search in four databases.
Study Selection
Observational studies reporting the prevalence of NS after BA in adult patients with CD.
Data extraction
Data extraction and risk of bias assessment were performed by three independent investigators.
Data synthesis
Thirty-six studies, with a total of 1316 CD patients treated with BA, were included for the primary outcome. Pooled prevalence of NS was 26% (95% CI 22–31%), with moderate to high heterogeneity (I2 67%, P < 0.01). The time from BA to NS varied from 2 months to 39 years. The prevalence of NS in the most recently published studies, where magnet resonance imaging was used, was 38% (95% CI 27–50%). The prevalence of treatment for NS was 21% (95% CI 18–26%). Relative risk for NS was not significantly affected by prior pituitary radiotherapy [0.9 (95% CI 0.5–1.6)] or pituitary surgery [0.6 (95% CI 0.4–1.0)].
Conclusions
Every fourth patient with CD treated with BA develops NS, and every fifth patient requires pituitary-specific treatment. The risk of NS may persist for up to four decades after BA. Life-long follow-up is essential for early detection and adequate treatment of NS.
Introduction
Cushing´s disease (CD) is a rare disorder associated with excess morbidity and increased mortality [1, 2]. Previously, bilateral adrenalectomy (BA) was the mainstay treatment for CD. During the last decades, however, other treatment modalities have emerged, including pituitary surgery, radiotherapy and medical treatments. Despite this, BA is still considered when other treatment options have failed to achieve remission, or when a rapid relief of hypercortisolism is necessary [3].
BA is considered to be a safe and effective treatment for CD [4], especially after the laparoscopic approach was introduced during the 1990s [5]. There are, however, significant drawbacks with BA, mainly the unavoidable chronic adrenal insufficiency, as well as the risk for Nelson’s syndrome (NS), i.e., growth of the remaining pituitary tumor and excessive production of ACTH, that may cause optic nerve or chiasmal compression and mucocutaneous hyperpigmentation [6].
The prevalence of NS varies between studies, mainly due to a lack of consensus on the definition and diagnostic criteria for the syndrome [7, 8]. Previously published studies are also inconsistent as to whether factors such as previous radiotherapy, age at BA, gender and duration of CD, may affect the risk of developing NS. Furthermore, high ACTH concentrations after BA have been suggested as a risk factor for developing NS [9,10,11,12].
Thus, the primary aim of this systematic review and meta-analysis was to estimate the prevalence of NS after BA for CD, both the total prevalence of NS as well the prevalence of NS requiring treatment with pituitary surgery and/or radiotherapy. The secondary aim was to investigate risk factors associated with development of NS.
Methods
A systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [13]. The PICO process was applied for the definition of the research question and eligibility criteria for the literature search. The protocol of this review was registered in the PROSPERO database (CRD42020163918).
Search strategy
We searched PubMed, Embase, Cochrane Library and Web of Science on February 25th 2020, with no start date restriction, for relevant articles by using the following terms: “Cushing´s syndrome” or “Cushing´s disease” or “Hypercortisolism” or “Pituitary ACTH hypersecretion” or “corticotroph tumor” or “corticotroph tumors” or “corticotroph adenoma” or “corticotroph adenomas” or “corticotropinoma” or “corticotropinomas” or “corticotrophinoma” or “corticotrophinomas” or “ACTH pituitary adenoma” or “ACTH pituitary adenomas” or “adrenocorticotropin pituitary adenoma” or “adrenocorticotropin pituitary adenomas” AND “bilateral adrenalectomy” or “bilateral adrenalectomies” or “total adrenalectomy” or “total adrenalectomies”. A detailed description of the search strategy is given in the Supplementary. Also, references of the included studies and relevant review articles were checked manually for additional articles. A new search was performed on January 12th 2021, prior submission, to identify any new publications.
Study selection and eligibility criteria
Eligible studies were observational studies (cohort or cross-sectional studies) reporting the prevalence of NS in adult patients with CD treated with BA. Studies including only children (age < 18 years), review articles, letters, commentaries and meeting abstracts were excluded. Moreover, case reports, case-series and studies with a population of fewer than 10 cases were excluded. Also, studies written in languages other than English were not considered for inclusion.
Data collection process and data extraction
Titles and abstracts from all identified articles were screened for eligibility and further full-text assessment by three independent investigators (EP, MP, OR). Discrepancies were resolved through discussion and consensus. Duplicate articles and studies with overlapping populations were excluded. In the latter case, the publication with the largest population, more comprehensive information on relevant clinical variables and/or lowest risk of bias was included.
Full-text assessment and data extraction were conducted independently by the same investigators as above. Data on the following predefined variables were extracted: first author, year of publication, region/hospital, study period, characteristics of the study population (number of patients, gender, follow-up, age at CD, age at BA, previous treatment with radiotherapy and/or pituitary surgery, ACTH concentrations at BA, MRI findings at CD and at BA), intervention (BA as primary or secondary treatment, remission status) and outcome (criteria for NS, number of patients with NS, age at NS, time from BA to NS, ACTH concentrations one year after BA, number of patients treated for NS, type of treatment; pituitary radiotherapy and/or pituitary surgery).
One of the studies included in the meta-analysis is our nationwide Swedish study on CD [2]. Additional clinical data, not provided in the original publication, was retrieved and used in the current analysis (Table 1).Table 1 Characteristics of the included studiesFull size table
Risk of bias assessment
The Newcastle–Ottawa Scale [14], modified to suit the current study, was used for assessment of risk of bias of all included studies. Three investigators (EP, MP, OR) assessed the studies independently, and any disagreements were resolved by discussion. Selection, comparability and outcome were assessed through predefined criteria. All studies that provided information on NS as outcome, and/or corticotroph tumor progression, were included, and the definition as well as the treatment of NS were recorded (Table 1 and Table S1). A clear definition of NS and information on treatment were considered to be two of the most important components of the quality assessment. We considered the definition of NS to be clear when it included either a new visible pituitary tumor or progression of a pituitary tumor remnant following BA, alone, or in combination with high ACTH concentrations and/or hyperpigmentation. Detailed description of the criteria for the risk of bias assessment is provided in the Supplementary file. Studies with an overall score ≥ 5 (max overall grade 8) and a clear definition of NS, were considered to have a low risk of bias.
Data synthesis and statistical analysis
Primary endpoints were the prevalence of NS, as well as the prevalence of pituitary-specific treatment for NS. Descriptive data are presented as median (range or interquartile range; IQR). Meta-analysis was performed by using the meta package in R (version 4.0.3) [15]. Statistical pooling was performed according to random-effects model due to the clinical heterogeneity among the included studies [16]. For all analyses, indices of heterogeneity, I2 statistics and Cochrane’s Q test, are reported. For the primary outcomes we estimated pooled prevalence with 95% confidence intervals (95% CI). Statistical significance was defined as P < 0.05. The possibility of publication bias was assessed by visual inspection of funnel plots as well as with the Egger’s test [17].
Sensitivity analyses were performed by excluding studies with an overall risk of bias < 5, and studies where information on diagnostic criteria for NS was lacking. By choosing the overall risk of bias < 5, all studies without adequate follow-up were also excluded (Table S2). Also, another sensitivity analysis was performed by including all studies reporting the number of patients with NS who received treatment for NS (Table 1).
Subgroup analyses were performed to investigate factors that may affect the prevalence of NS, namely pituitary radiotherapy prior to BA, prophylactic pituitary radiotherapy, overall radiotherapy (prior to BA or prophylactic), pituitary surgery (transcranial or transsphenoidal surgery) prior to BA, and BA as primary or secondary treatment. For these outcomes, we estimated relative risks (RRs), or pooled prevalence, with 95% CIs. Also, in a subgroup analysis, the prevalence (with 95% CI) of NS and treatment for NS were estimated in studies where MRI was used at diagnosis and during follow-up.
Uni- and bivariate meta-regression was used to investigate whether the prevalence of NS was influenced by median follow-up time or age at BA. The meta-analysis was performed by using the Metareg command in R. The estimated association is reported as β coefficient.
Role of funding source
The funding source had no role in the design and conduction of the study; i.e., collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Results
Identification and description of included studies
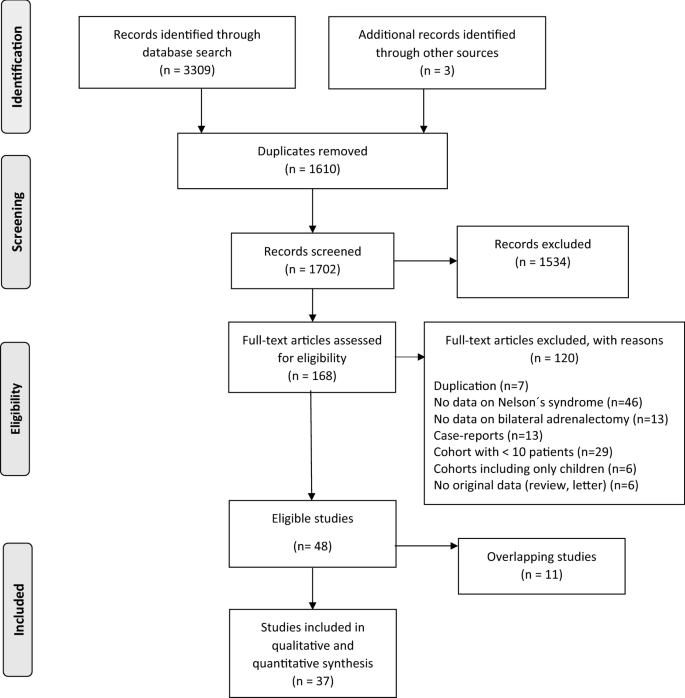
After removal of duplicates, 1702 articles were identified (Fig. 1). Three additional articles were found after checking the reference lists of identified articles and review papers. After reviewing titles, abstracts and full-text articles, 48 articles were considered eligible for further analysis. Of these, however, 11 articles were excluded due to overlapping or identical patient cohorts. Thus, 37 studies published between 1976 and 2020, were included in the current meta-analysis (Fig. 1). All studies had a retrospective observational design. Characteristics of the included studies are presented in Table 1. Two of the included studies had an overlapping cohort where one was used for the main outcome [18] and one [19] for the subgroup analyses on the influence of radiotherapy on the development of NS. An overview of risk of bias assessment of the eligible studies is provided in Table S2.
Fig. 1
In total, 1316 patients with CD treated with BA were included. The median follow-up after BA was 7 years (23 studies, range 3.3–22). Median age at BA in patients with NS was 31 years (13 studies, IQR 26–34). Median time from BA to the diagnosis of NS was 4 years (19 studies) with the shortest reported time being 2 months [20] and the longest 39 years [2]. At diagnosis of NS, hyperpigmentation was reported in 155 of 188 (82%) patients (19 studies) and chiasmal compression in 24 of 129 (19%) patients [11 studies].
Prevalence of NS
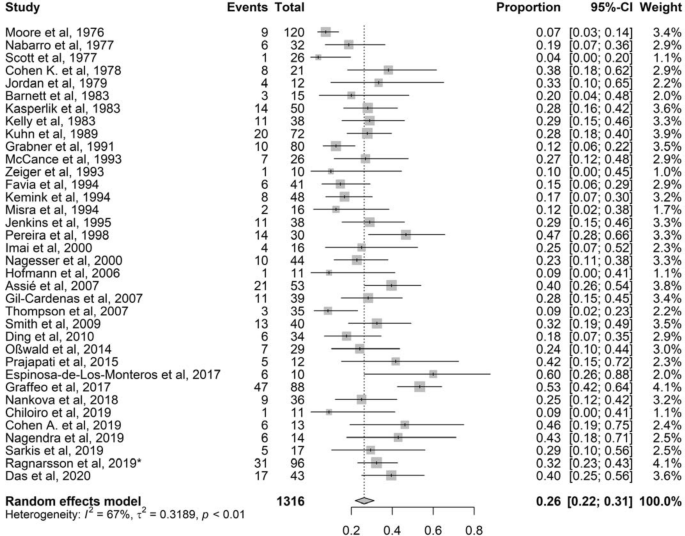
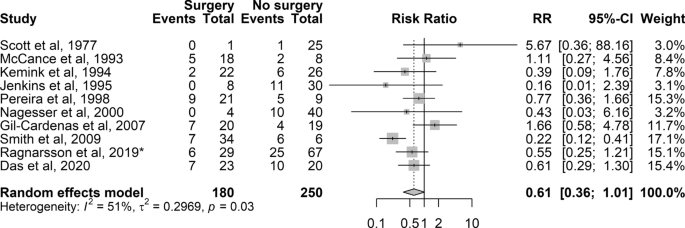
Thirty-six of 37 studies, with total 1316 patients with CD treated with BA, were included [2, 18, 20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53]. Reported prevalence of NS ranged from 4 to 60%. The mean pooled prevalence was 26% (95% CI 22–31%) with a moderate to high heterogeneity (I2 67%, P < 0.01) (Fig. 2). The Egger’s test was statistically significant (P = 0.01), but visual inspection showed no obvious asymmetry. The significant Egger’s test indicates publication bias, probably explained by the fact that case reports and cohorts with fewer than 10 participants were excluded (Fig. S1).
Fig. 2
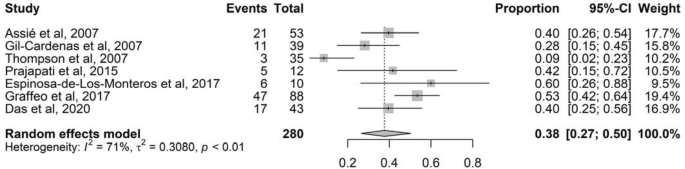
In a sensitivity analysis, excluding all studies with high risk of bias (overall score < 5) and no clear definition of NS, the pooled prevalence was 31% (95% CI 24–38%; I2 76%, 17 studies, 822 patients; P < 0.01) (Fig. S2). In a subgroup analysis, the prevalence of NS in studies where MRI was used at diagnosis and during follow-up was 38% (Fig. 3; 95% CI 27–50%; I2 71%, 7 studies, 280 patients; P < 0.01).
Fig. 3
Prevalence of treated NS
The pooled prevalence of treatment for NS was 21% (95% CI 18–26%; I2 52%, P < 0.01) (Table 1; 29 studies with 1074 patients). Thus, the pooled prevalence was slightly lower, compared to the pooled prevalence of NS in total, as well as the heterogeneity (Fig. S3). The funnel plot showed no asymmetry and Egger’s test was not statistically significant, indicating low possibility of publication bias (Fig. S4). In a subgroup analysis, the prevalence of treated NS in studies where MRI was used at diagnosis and during follow-up was 25% (95% CI 17–35%; I2 61%, 7 studies; P = 0.02).
The indication for treatment was progression of the pituitary tumor in 23 out of 28 patients (82%, five studies), optic chiasmal compression in 11 out of 91 patients (12%, 11 studies), while four patients out of 14 (one study) had both these indications for treatment. Twenty-six studies provided information on treatment modalities (pituitary surgery and/or radiotherapy). Seventy-three out of 201 patients with NS (36%) were treated with pituitary surgery, 86 (43%) with radiotherapy and 41 (20%) received both treatments.
Radiotherapy
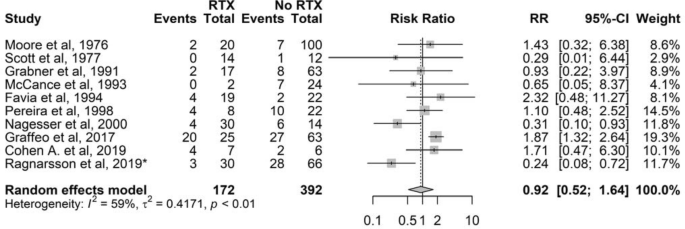
Nineteen studies provided information on radiotherapy prior to BA. However, nine studies had no events and no patients in one of the arms (radiotherapy or no radiotherapy) (Table S3). Thus, ten studies were eligible for further estimation, showing that the risk for NS in patients treated with radiotherapy prior to BA was comparable to the risk in patients not treated with radiotherapy (RR 0.9, 95% CI 0.5–1.6; 10 studies with 564 patients) (Fig. 4).
Fig. 4
Thirteen studies provided information on prophylactic radiotherapy. However, only one study provided applicable data for calculating RR, thus subgroup analysis was not performed (Table S4). In that study [20], none of the seventeen patients who received prophylactic radiotherapy developed NS, while 11 of 22 patients without radiotherapy developed NS after a mean follow-up of 4.4 years (range 10–16 years).
By using studies with information on either previous or prophylactic radiotherapy (11 studies with 603 patients; Table S5), the pooled RR was 0.8 (95% CI 0.5–1.5).
Pituitary surgery prior to BA
Of 21 studies with information on pituitary surgery prior to BA (Table S6), only ten provided information for estimation of RR. A pooled RR of 0.6 (10 studies with 430 patients; 95% CI 0.4–1.0) was found (Fig. 5), indicating that the risk for developing NS was not influenced by previous pituitary surgery.
Fig. 5
BA as primary or secondary treatment for CD
Information on whether patients with NS were treated primarily with BA or not, was provided in ten and nine studies, respectively (Fig. S5 and S6). The pooled prevalence of NS was 26% (95% CI 20–33%) for patients treated primarily with BA and 22% (95% CI 15–31%) for patients who had been treated with pituitary surgery and/or radiotherapy prior to BA.
ACTH concentrations one year after BA
Four studies provided information on ACTH concentrations during the first year after BA [45, 49, 52, 53]. In a study by Assié et al. the median ACTH concentration in patients who developed NS was 301 pmol/L, compared to 79 pmol/L in patients without NS (upper range of limit; URL 13 pmol/L) [52]. The median ACTH concentration in a study by Cohen et al. was 105 pmol/L in the NS group compared to 18 pmol/L in patients without NS (P = 0.007) (URL 10 pmol/L) [49]. Also, in a study by Das et al., there was a statistically significant difference in ACTH concentrations one year after BA between patients with and without NS (110 vs 21 pmol/L respectively; P = 0.002) [53]. On the contrary, Espinosa-de-Los-Monteros et al.found no difference in ACTH concentrations between the patients with NS and those without NS [45]. Thus, three of four studies found that high ACTH concentrations one year after BA were associated with the development of NS. However, since the ACTH assays and the conditions when ACTH was collected were different in these studies (Table S7), further comparison or a meta-analysis on ACTH levels after BA was not considered feasible.
Influence of age at BA and duration of follow-up on prevalence of NS
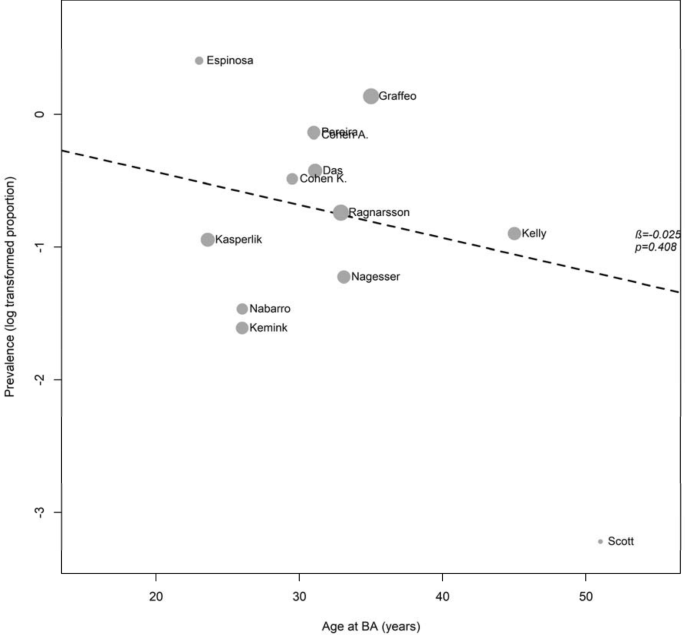
In a meta-regression analysis, age at BA (β-coefficient = – 0.03, P = 0.4; Fig. 6) and median duration of follow-up (β-coefficient = 0.01, P = 0.7; Fig. S7) were not associated with prevalence of NS. After adjustment for follow-up, age at BA was still not associated with prevalence of NS (β-coefficient = -0.03, P = 0.4).
Fig. 6
Discussion
In this study we have for the first time evaluated the pooled prevalence of NS by using a meta-analysis on data from 36 studies, including more than 1300 patients with CD treated with BA. The overall prevalence of NS was 26% and the median time from BA to diagnosis of NS was 4 years, ranging from 0.2 to 39 years. The prevalence of patients requiring pituitary-specific treatment for NS was 21%. Furthermore, radiotherapy and pituitary surgery prior to BA, as well as age at BA, did not seem to affect the risk of developing NS.
Various definitions have been used for NS over the past decades [12]. Historically, the diagnosis was based on clinical findings related to mucocutaneous hyperpigmentation and chiasmal compression, together with signs of an enlarged sella turcica on skull radiography [6]. Since then, the diagnosis of NS in most studies has been based on (i) radiological evidence of a pituitary tumor that becomes visible, or a progression of a preexisting tumor, (ii) “high” ACTH concentrations, and (iii) hyperpigmentation [54]. In the studies with the highest prevalence of NS [45, 46], the diagnosis was based on rising ACTH concentrations and an expanding pituitary mass, where 2 mm increment in tumor size on MRI was considered to be a significant growth. On the contrary, the criteria for NS in studies with the lowest prevalence were based on hyperpigmentation, often but not always combined with a pituitary tumor responding to radiotherapy and/or a radiographic evidence of pituitary tumor on skull radiography [21, 23]. Thus, the great variance in the prevalence of NS between studies can, at least partly, be explained by the different definitions of NS. Consequently, in an expert opinion published in 2010, it was suggested that the diagnosis of NS should be based on an elevated level of ACTH >500 ng/L (110 pmol/L) in addition to rising levels of ACTH on at least three consecutive occasions and/or an expanding pituitary mass on MRI or CT following BA [54]. Similarly, in a recently published expert consensus recommendation, based on a systematic review, it was suggested that NS should be defined as radiological progression or new detection of a pituitary tumor on a thin-section MRI [55]. Furthermore, the authors recommend active surveillance with MRI three months after BA, and every 12 months for the first 3 years, and every 2–4 years thereafter, based on clinical findings. The meta-regression of the current analysis did not show an association between median follow-up time and prevalence of NS. Nevertheless, NS occurred as early as 2 months [20], and up to 39 years after BA [2], supporting that life-long surveillance after BA is necessary for patients with CD.
Active surveillance with MRI was more common in studies published during the last two decades. In fact, the use of MRI in recent studies resulted in earlier detection of a growing pituitary adenoma and, subsequently, contributed to a higher prevalence of NS. Namely, the seven studies including patients treated with BA after 1990 and using MRI reported higher prevalence of NS, both overall NS and treated NS.
Whether factors such as pituitary radiotherapy affects the risk for development of NS has been evaluated in several studies. Some studies have shown that radiotherapy prior to BA, or administrated prophylactically, can prevent or delay the development of NS [20, 39]. On the contrary, other studies have not demonstrated a protective effect of radiotherapy prior to BA [18, 37] and, moreover, one study found an association with tumor progression [46]. Nevertheless, the current meta-analysis indicates that radiotherapy prior to BA does not decrease the risk of developing NS. Neither did previous pituitary surgery affect the risk for NS.
Elevated ACTH concentrations during the first year after BA have been considered to be a strong predictor of NS [49, 52]. In fact, seven studies in the current analysis included cut-off levels for ACTH concentration, arbitrarily defined, for the diagnosis of NS [18, 25, 34, 36, 41, 45, 49]. Due to the different ACTH assays, and different conditions when ACTH was collected, no further analysis on ACTH levels was performed. Nevertheless, four studies [45, 49, 52, 53] reported ACTH concentrations one year after BA in both patients with and without NS. Three of these studies found that high ACTH concentrations one year after BA [49, 52, 53] were associated with pituitary tumor progression. Thus, these findings support the suggestion that ACTH should be monitored following BA in patients with CD [54, 55].
The prevalence of treatment for NS (21%), and the heterogeneity index (52%), were slightly lower than in the analysis of total prevalence of NS (26%, I2 67%). The majority of the patients was treated with radiotherapy, followed by pituitary surgery and combination of pituitary surgery and radiotherapy. Today, surgical removal of the pituitary tumor is considered to be the first-line therapy of NS whereas radiotherapy is considered if surgery has failed or is not possible [12, 54, 56]. In a large multi-center study by Fountas et al., the 10-year progression-free survival rates after surgery alone, or with radiotherapy, for patients with NS was 80% and 81%, respectively [57]. In comparison, progression-free survival rate in patients who did not receive treatment was 51%. Reports on the efficacy of medical therapy for NS have shown inconsistent results [56].
Strengths and limitations
This is the largest systematic review, and the first meta-analysis, on NS published to date. However, some limitations have to be acknowledged. Most important are the different diagnostic methods used to detect NS, and the different definitions of the syndrome between the studies. The majority of the studies have used the combination of hyperpigmentation, high ACTH concentrations and radiological findings for the diagnosis of NS. Notwithstanding these common criteria, there were still differences in the cut-offs of ACTH levels, the use of different radiological modalities over time as well as the radiological definition of progress of pituitary tumors. Moreover, in some studies radiological findings were used solely or in combination with either hyperpigmentation and/or bitemporal hemianopsia, ACTH concentrations or response to treatment of NS. Furthermore, in several studies a clear definition of NS was not provided. Nevertheless, we consider our attempt to address the heterogeneity of the included studies, through systematic review, quality assessment, and sensitivity and subgroup analyses to be a strength.
Conclusions
The risk of NS after BA in patients with CD is considerable and may first become clinically evident many decades later. Thus, life-long close follow-up is necessary for an early detection of a growing pituitary tumor, and adequate treatment when needed. Although this meta-analysis did not find prior surgery or radiotherapy to be associated with risk of NS, the findings are based on a limited number of studies. Thus, in order to individualize the treatment for patients with CD, further studies are needed where these and other factors possibly associated with risk of NS are evaluated.
Data availability
The data generated or analyzed during this study are included in this published article or in the Supplementary file.
Abbreviations
CD:
Cushing’s diseaseBA:
Bilateral adrenalectomyNS:
Nelson’s syndromeACTH:
Adrenocorticotropic hormoneRR:
Relative riskMRI:
Magnet resonance imagingCT:
Computer tomography
References
1.Papakokkinou E, Olsson DS, Chantzichristos D, Dahlqvist P, Segerstedt E, Olsson T, Petersson M, Berinder K, Bensing S, Hoybye C, Eden-Engstrom B, Burman P, Bonelli L, Follin C, Petranek D, Erfurth EM, Wahlberg J, Ekman B, Akerman AK, Schwarcz E, Bryngelsson IL, Johannsson G, Ragnarsson O (2020) Excess morbidity persists in patients with cushing’s disease during long-term remission: a swedish nationwide study. J Clin Endocrinol Metab 105(8):2616–2624
2.Ragnarsson O, Olsson DS, Papakokkinou E, Chantzichristos D, Dahlqvist P, Segerstedt E, Olsson T, Petersson M, Berinder K, Bensing S, Hoybye C, Eden-Engstrom B, Burman P, Bonelli L, Follin C, Petranek D, Erfurth EM, Wahlberg J, Ekman B, Akerman AK, Schwarcz E, Bryngelsson IL, Johannsson G (2019) Overall and disease-specific mortality in patients with cushing disease: a swedish nationwide study. J Clin Endocrinol Metab 104(6):2375–2384PubMedArticleGoogle Scholar
3.Nieman LK, Biller BM, Findling JW, Murad MH, Newell-Price J, Savage MO, Tabarin A, Endocrine S (2015) Treatment of cushing’s syndrome: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 100(8):2807–2831CASPubMedPubMed CentralArticleGoogle Scholar
4.Ritzel K, Beuschlein F, Mickisch A, Osswald A, Schneider HJ, Schopohl J, Reincke M (2013) Clinical review: outcome of bilateral adrenalectomy in Cushing’s syndrome: a systematic review. J Clin Endocrinol Metab 98(10):3939–3948CASPubMedArticleGoogle Scholar
5.Reincke M, Ritzel K, Osswald A, Berr C, Stalla G, Hallfeldt K, Reisch N, Schopohl J, Beuschlein F (2015) A critical reappraisal of bilateral adrenalectomy for ACTH-dependent Cushing’s syndrome. Eur J Endocrinol 173(4):M23-32CASPubMedArticleGoogle Scholar
6.Nelson DH, Meakin JW, Dealy JB Jr, Matson DD, Emerson K Jr, Thorn GW (1958) ACTH-producing tumor of the pituitary gland. N Engl J Med 259(4):161–164CASPubMedArticleGoogle Scholar
7.Guerin C, Taieb D, Treglia G, Brue T, Lacroix A, Sebag F, Castinetti F (2016) Bilateral adrenalectomy in the 21st century: when to use it for hypercortisolism? Endocr Relat Cancer 23(2):R131-142CASPubMedArticleGoogle Scholar
8.Katznelson L (2015) Bilateral adrenalectomy for Cushing’s disease. Pituitary 18(2):269–273CASPubMedArticleGoogle Scholar
9.Banasiak MJ, Malek AR (2007) Nelson syndrome: comprehensive review of pathophysiology, diagnosis, and management. Neurosurg Focus 23(3):E13PubMedArticleGoogle Scholar
10.Assie G, Bahurel H, Bertherat J, Kujas M, Legmann P, Bertagna X (2004) The Nelson’s syndrome revisited. Pituitary. 7(4):209–215PubMedArticleGoogle Scholar
11.Ragnarsson O (2020) Cushing’s syndrome disease monitoring: recurrence, surveillance with biomarkers or imaging studies. Best Pract Res Clin Endocrinol Metab. 34(2):101382PubMedArticleGoogle Scholar
12.Fountas A, Karavitaki N (2020) Nelson’s syndrome: an update. Endocrinol Metab Clin North Am 49(3):413–432PubMedArticleGoogle Scholar
13.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097PubMedPubMed CentralArticleGoogle Scholar
15.Balduzzi S, Rucker G, Schwarzer G (2019) How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health 22(4):153–160PubMedArticleGoogle Scholar
16.Lau J, Ioannidis JP, Schmid CH (1998) Summing up evidence: one answer is not always enough. Lancet 351(9096):123–127CASPubMedArticleGoogle Scholar
17.Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315(7109):629–634CASPubMedPubMed CentralArticleGoogle Scholar
18.Smith PW, Turza KC, Carter CO, Vance ML, Laws ER, Hanks JB (2009) Bilateral adrenalectomy for refractory Cushing disease: a safe and definitive therapy. J Am Coll Surg 208(6):1059–1064PubMedArticleGoogle Scholar
19.Mehta GU, Sheehan JP, Vance ML (2013) Effect of stereotactic radiosurgery before bilateral adrenalectomy for Cushing’s disease on the incidence of Nelson’s syndrome. J Neurosurg 119(6):1493–1497PubMedArticleGoogle Scholar
20.Gil-Cardenas A, Herrera MF, Diaz-Polanco A, Rios JM, Pantoja JP (2007) Nelson’s syndrome after bilateral adrenalectomy for Cushing’s disease. Surgery. 141(2):147–151
21.Moore TJ, Dluhy RG, Williams GH, Cain JP (1976) Nelson’s syndrome: frequency, prognosis, and effect of prior pituitary irradiation. Ann Intern Med 85(6):731–734CASPubMedArticleGoogle Scholar
24.Cohen KL, Noth RH, Pechinski T (1978) Incidence of pituitary tumors following adrenalectomy. A long-term follow-up study of patients treated for Cushing’s disease. Arch Internal Med 138(4):575–579CASArticleGoogle Scholar
26.Barnett AH, Livesey JH, Friday K, Donald RA, Espiner EA (1983) Comparison of preoperative and postoperative ACTH concentrations after bilateral adrenalectomy in Cushing’s disease. Clin Endocrinol (Oxf) 18(3):301–305CASArticleGoogle Scholar
28.Kelly WF, MacFarlane IA, Longson D, Davies D, Sutcliffe H (1983) Cushing’s disease treated by total adrenalectomy: long-term observations of 43 patients. Q J Med 52(206):224–231CASPubMedGoogle Scholar
29.Kuhn JM, Proeschel MF, Seurin DJ, Bertagna XY, Luton JP, Girard FL (1989) Comparative assessment of ACTH and lipotropin plasma levels in the diagnosis and follow-up of patients with Cushing’s syndrome: a study of 210 cases. Am J Med 86(6 Pt 1):678–684CASPubMedArticleGoogle Scholar
30.Grabner P, Hauerjensen M, Jervell J, Flatmark A (1991) Long-term results of treatment of cushings-disease by adrenalectomy. Acta Chirurgica- Eur J Surgery 157(8):461–464CASGoogle Scholar
31.McCance DR, Russell CF, Kennedy TL, Hadden DR, Kennedy L, Atkinson AB (1993) Bilateral adrenalectomy: low mortality and morbidity in Cushing’s disease. Clin Endocrinol 39(3):315–321CASArticleGoogle Scholar
32.Zeiger MA, Fraker DL, Pass HI, Nieman LK, Cutler GB Jr, Chrousos GP, Norton JA (1993) Effective reversibility of the signs and symptoms of hypercortisolism by bilateral adrenalectomy. Surgery 114(6):1138–1143CASPubMedGoogle Scholar
33.Favia G, Boscaro M, Lumachi F, D’Amico DF (1994) Role of bilateral adrenalectomy in Cushing’s disease. World J Surg 18(4):462–466CASPubMedArticleGoogle Scholar
34.Kemink L, Pieters G, Hermus A, Smals A, Kloppenborg P (1994) Patient’s age is a simple predictive factor for the development of Nelson’s syndrome after total adrenalectomy for Cushing’s disease. J Clin Endocrinol Metab 79(3):887–889CASPubMedGoogle Scholar
35.Misra D, Kapur MM, Gupta DK (1994) Incidence of Nelson’s syndrome and residual adrenocortical function in patients of Cushing’s disease after bilateral adrenalectomy. J Assoc Physicians India 42(4):304–305CASPubMedGoogle Scholar
36.Jenkins PJ, Trainer PJ, Plowman PN, Shand WS, Grossman AB, Wass JA, Besser GM (1995) The long-term outcome after adrenalectomy and prophylactic pituitary radiotherapy in adrenocorticotropin-dependent Cushing’s syndrome. J Clin Endocrinol Metab 80(1):165–171CASPubMedGoogle Scholar
37.Pereira MA, Halpern A, Salgado LR, Mendonca BB, Nery M, Liberman B, Streeten DH, Wajchenberg BL (1998) A study of patients with Nelson’s syndrome. Clin Endocrinol (Oxf) 49(4):533–539CASArticleGoogle Scholar
38.Imai T, Kikumori T, Funahashi H, Nakao A (2000) Surgical management of Cushing’s syndrome. Biomed Pharmacother 54(1):140–145ArticleGoogle Scholar
39.Nagesser SK, van Seters AP, Kievit J, Hermans J, Krans HM, van de Velde CJ (2000) Long-term results of total adrenalectomy for Cushing’s disease. World J Surg 24(1):108–113CASPubMedArticleGoogle Scholar
40.Hofmann BM, Fahlbusch R (2006) Treatment of Cushing’s disease: A retrospective clinical study of the latest 100 cases. Pituitary Surgery – A Modern Approach 34:158–184ArticleGoogle Scholar
41.Thompson SK, Hayman AV, Ludlam WH, Deveney CW, Loriaux DL, Sheppard BC (2007) Improved quality of life after bilateral laparoscopic adrenalectomy for Cushing’s disease: a 10-year experience. Ann Surg 245(5):790–794PubMedPubMed CentralArticleGoogle Scholar
42.Ding XF, Li HZ, Yan WG, Gao Y, Li XQ (2010) Role of adrenalectomy in recurrent Cushing’s disease. Chin Med J 123(13):1658–1662PubMedGoogle Scholar
43.Osswald A, Plomer E, Dimopoulou C, Milian M, Blaser R, Ritzel K, Mickisch A, Knerr F, Stanojevic M, Hallfeldt K, Schopohl J, Kuhn KA, Stalla G, Beuschlein F, Reincke M (2014) Favorable long-term outcomes of bilateral adrenalectomy in Cushing’s disease. Eur J Endocrinol 171(2):209–215CASPubMedArticleGoogle Scholar
44.Prajapati OP, Verma AK, Mishra A, Agarwal G, Agarwal A, Mishra SK (2015) Bilateral adrenalectomy for Cushing’s syndrome: pros and cons. Indian J Endocrinol Metabol 19(6):834–840CASArticleGoogle Scholar
45.Espinosa-de-Los-Monteros AL, Sosa-Eroza E, Espinosa E, Mendoza V, Arreola R, Mercado M (2017) Long-term outcome of the different treatment alternatives for recurrent and persistent cushing disease. Endocrine Pract: Off J Am College Endocrinol Am Assoc Clin Endocrinol 23(7):759–767ArticleGoogle Scholar
46.Graffeo CS, Perry A, Carlstrom LP, Meyer FB, Atkinson JLD, Erickson D, Nippoldt TB, Young WF, Pollock BE, Van Gompel JJ (2017) Characterizing and predicting the Nelson-Salassa syndrome. J Neurosurg 127(6):1277–1287CASPubMedArticleGoogle Scholar
47.Nankova A, Yaneva M, Elenkova A, Tcharaktchiev D, Marinov M, Hadzhiyanev A, Sechanov T, Gantchev G, Todorov G, Kirilov G, Kalinov K, Andreeva M, Zacharieva S (2018) Cushing’s syndrome: a historic review of the treatment strategies and corresponding outcomes in a single tertiary center over the past half-century. Hormone Metab Res 50(4):280–289CASArticleGoogle Scholar
48.Chiloiro S, Giampietro A, Raffaelli M, D’Amato G, Bima C, Lauretti L, Anile C, Lombardi CP, Rindi G, Bellantone R, De Marinis L, Pontecorvi A, Bianchi A (2019) Synchronous bilateral adrenalectomy in ACTH-dependent hypercortisolism: predictors, biomarkers and outcomes. Endocrine 66(3):642–649CASPubMedArticleGoogle Scholar
49.Cohen AC, Goldney DC, Danilowicz K, Manavela M, Rossi MA, Gomez RM, Cross GE, Bruno OD (2019) Long-term outcome after bilateral adrenalectomy in Cushing’s disease with focus on Nelson’s syndrome. Arch Endocrinol Metab 63(5):470–477
50.Nagendra L, Bhavani N, Pavithran PV, Kumar GP, Menon UV, Menon AS, Kumar L, Kumar H, Nair V, Abraham N, Narayanan P (2019) Outcomes of bilateral adrenalectomy in Cushing’s syndrome. Indian J Endocrinol Metab 23(2):193–197PubMedPubMed CentralArticleGoogle Scholar
51.Sarkis P, Rabilloud M, Lifante JC, Siamand A, Jouanneau E, Gay E, Chaffanjon P, Chabre O, Raverot G (2019) Bilateral adrenalectomy in Cushing’s disease: altered long-term quality of life compared to other treatment options. Ann Endocrinol 80(1):32–37ArticleGoogle Scholar
52.Assie G, Bahurel H, Coste J, Silvera S, Kujas M, Dugue MA, Karray F, Dousset B, Bertherat J, Legmann P, Bertagna X (2007) Corticotroph tumor progression after adrenalectomy in Cushing’s disease: a reappraisal of Nelson’s Syndrome. J Clin Endocrinol Metab 92(1):172–179CASPubMedArticleGoogle Scholar
53.Das L, Bhansali A, Pivonello R, Dutta P, Bhadada SK, Ahuja CK, Mavuduru R, Kumar S, Behera A, Saikia UN, Dhandapani S, Walia R (2020) ACTH increment post total bilateral adrenalectomy for Cushing’s disease: a consistent biosignature for predicting Nelson’s syndrome. Pituitary 23(5):488–497CASPubMedArticleGoogle Scholar
54.Barber TM, Adams E, Ansorge O, Byrne JV, Karavitaki N, Wass JA (2010) Nelson’s syndrome. Eur J Endocrinol 163(4):495–507CASPubMedArticleGoogle Scholar
55.Reincke M, Albani A, Assie G, Bancos I, Brue T, Buchfelder M, Chabre O, Ceccato F, Daniele A, Detomas M, Di Dalmazi G, Elenkova A, Findling J, Grossman AB, Gomez-Sanchez CE, Heaney AP, Honegger J, Karavitaki N, Lacroix A, Laws ER, Losa M, Murakami M, Newell-Price J, Pecori Giraldi F, Perez-Rivas LG, Pivonello R, Rainey WE, Sbiera S, Schopohl J, Stratakis CA, Theodoropoulou M, van Rossum EFC, Valassi E, Zacharieva S, Rubinstein G, Ritzel K (2021) Corticotroph tumor progression after bilateral adrenalectomy (Nelson’s syndrome): systematic review and expert consensus recommendations. Eur J Endocrinol. https://doi.org/10.1530/EJE-20-1088
56.Patel J, Eloy JA, Liu JK (2015) Nelson’s syndrome: a review of the clinical manifestations, pathophysiology, and treatment strategies. Neurosurg Focus 38(2):E14PubMedArticleGoogle Scholar
57.Fountas A, Lim ES, Drake WM, Powlson AS, Gurnell M, Martin NM, Seejore K, Murray RD, MacFarlane J, Ahluwalia R, Swords F, Ashraf M, Pal A, Chong Z, Freel M, Balafshan T, Purewal TS, Speak RG, Newell-Price J, Higham CE, Hussein Z, Baldeweg SE, Dales J, Reddy N, Levy MJ, Karavitaki N (2020) Outcomes of patients with Nelson’s syndrome after primary treatment: a multicenter study from 13 UK pituitary centers. J Clin Endocrinol Metab 105(5):1527–1537
We would like to thank Therese Svanberg, librarian at the Medical Library at Sahlgrenska University Hospital for her expert assistance with the literature search.
Funding
Open access funding provided by University of Gothenburg. The study was financed by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement (ALFGBG-593301) and a grant from the Gothenburg Society of Medicine.
Author information
Affiliations
Department of Internal Medicine and Clinical Nutrition, Institute of Medicine at Sahlgrenska Academy, University of Gothenburg, 413 45, Gothenburg, SwedenEleni Papakokkinou, Marta Piasecka, Dimitrios Chantzichristos, Daniel S. Olsson, Gudmundur Johannsson & Oskar Ragnarsson
The Department of Endocrinology, Sahlgrenska University Hospital, Blå stråket 5, 413 45, Gothenburg, SwedenEleni Papakokkinou, Marta Piasecka, Dimitrios Chantzichristos, Daniel S. Olsson, Gudmundur Johannsson & Oskar Ragnarsson
Department of Environmental and Occupational Health School of Public Health and Community Medicine, University of Gothenburg, 4053, Gothenburg, SwedenHanne Krage Carlsen
Department of Public Health and Clinical Medicine, Umeå University, 901 87, Umeå, SwedenPer Dahlqvist
Department of Molecular Medicine and Surgery, Karolinska Institutet, 17176, Stockholm, SwedenMaria Petersson, Katarina Berinder, Sophie Bensing, Charlotte Höybye & Henrik Falhammar
Department of Endocrinology, Karolinska University Hospital, 171 76, Stockholm, SwedenMaria Petersson, Katarina Berinder, Sophie Bensing, Charlotte Höybye & Henrik Falhammar
Department of Endocrinology and Diabetes, Uppsala University Hospital, and Department of Medical Sciences, Endocrinology and Mineral Metabolism, Uppsala University, 751 85, Uppsala, SwedenBritt Edén Engström
Department of Endocrinology, Skåne University Hospital, University of Lund, 205 02, Malmö, SwedenPia Burman
Department of Endocrinology, Skåne University Hospital, 222 42, Lund, SwedenCecilia Follin, David Petranek & Eva Marie Erfurth
Department of Endocrinology and Department of Medical and Health Sciences, Linköping University, 581 83, Linköping, SwedenJeanette Wahlberg & Bertil Ekman
Department of Internal Medicine, School of Health and Medical Sciences, Örebro University, 702 81, Örebro, SE, SwedenJeanette Wahlberg, Anna-Karin Åkerman & Erik Schwarcz
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Papakokkinou, E., Piasecka, M., Carlsen, H.K. et al. Prevalence of Nelson’s syndrome after bilateral adrenalectomy in patients with cushing’s disease: a systematic review and meta-analysis. Pituitary (2021). https://doi.org/10.1007/s11102-021-01158-z
High blood sugar or glucose, also called hyperglycemia, occurs when there is too much sugar in the blood. High blood sugar is the primary symptom that underlies diabetes, but it can also occur in people who don’t have type 1 or type 2 diabetes, either because of stress or trauma, or gradually as a result of certain chronic conditions.
It is important to manage high blood sugar, even if you don’t have diabetes, because elevated blood glucose can delay your ability to heal, increase your risk of infections, and cause irreversible damage to your nerves, blood vessels, and organs, such as your eyes and kidneys. Blood vessel damage from high blood sugar also increases your risk of heart attack and stroke.
Non-Diabetic Hyperglycemia and Prediabetes
You are considered to have impaired glucose tolerance or prediabetes if you have a fasting glucose level between 100–125 mg/dL, and hyperglycemia if your fasting blood glucose level is greater than 125 mg/dL, or greater than 180 mg/dL one to two hours after eating.
The body obtains glucose mainly through carbohydrate consumption, but also through the breakdown of glycogen to glucose—a process called glycogenolysis—or conversion of non-carbohydrate sources to glucose—called gluconeogenesis—that primarily occurs in the liver.
While 50% to 80% of glucose is used by the brain, kidneys, and red blood cells for energy, the remaining supply of glucose is used to produce energy. It is stored as glycogen in the liver and muscles, and can be tapped into at a later time for energy or converted into fat tissue.
In healthy people, blood glucose levels are regulated by the hormone insulin to stay at a steady level of 80–100 mg/dL. Insulin maintains steady blood sugar by increasing the uptake and storage of glucose and decreasing inflammatory proteins that raise blood sugar when there is an excess of glucose in the blood.
Certain conditions can increase your blood glucose levels by impairing the ability of insulin to transport glucose out of the bloodstream. When this occurs, you develop hyperglycemia, which puts you at an increased risk of prediabetes, diabetes, and related complications.
Common Causes
Cushing’s Syndrome
Cushing’s syndrome results from excess secretion of the adrenocorticotropic hormone, a hormone produced in the anterior portion of the pituitary gland that causes excess cortisol to be produced and released from the adrenal glands. Pituitary adenomas, or tumors of the pituitary gland, are the cause of Cushing’s syndrome in more than 70% of cases, while prolonged use of corticosteroid medication can also significantly increase the risk.
People with Cushing’s syndrome are at an increased risk of developing impaired glucose tolerance and hyperglycemia as a result of increased levels of cortisol throughout the body. Cortisol is a hormone that counteracts the effects of insulin by blocking the uptake of glucose from the bloodstream, thereby increasing insulin resistance and maintaining high blood sugar levels. Elevated cortisol levels also partially decrease the release of insulin from where it is produced in the pancreas.
Approximately 10% to 30% of people with Cushing’s syndrome will develop impaired glucose tolerance, while 40% to 45% will develop diabetes.
Corticosteroid medication is often prescribed to decrease inflammation throughout the body, but can lead to the development of Cushing’s syndrome and hyperglycemia because it activates specific enzymes that increase the conversion of non-carbohydrate molecules into glucose (gluconeogenesis). Corticosteroids also disrupt pancreatic cell function by inhibiting cell signaling pathways involved in the release of insulin from the pancreas.
Endocrinol Diabetes Metab Case Rep. 2021 May 1;2021:EDM210038. doi: 10.1530/EDM-21-0038. Online ahead of print.
ABSTRACT
SUMMARY: In this case report, we describe the management of a patient who was admitted with an ectopic ACTH syndrome during the COVID pandemic with new-onset type 2 diabetes, neutrophilia and unexplained hypokalaemia. These three findings when combined should alert physicians to the potential presence of Cushing’s syndrome (CS). On admission, a quick diagnosis of CS was made based on clinical and biochemical features and the patient was treated urgently using high dose oral metyrapone thus allowing delays in surgery and rapidly improving the patient’s clinical condition. This resulted in the treatment of hyperglycaemia, hypokalaemia and hypertension reducing cardiovascular risk and likely risk for infection. Observing COVID-19 pandemic international guidelines to treat patients with CS has shown to be effective and offers endocrinologists an option to manage these patients adequately in difficult times.
LEARNING POINTS: This case report highlights the importance of having a low threshold for suspicion and investigation for Cushing’s syndrome in a patient with neutrophilia and hypokalaemia, recently diagnosed with type 2 diabetes especially in someone with catabolic features of the disease irrespective of losing weight. It also supports the use of alternative methods of approaching the diagnosis and treatment of Cushing’s syndrome during a pandemic as indicated by international protocols designed specifically for managing this condition during Covid-19.