


Abstract
Background
Objective
Methods
Results
Conclusion
Abbreviations
Highlights
- •
Reflexing only nonsuppressed serum cortisol samples for the measurement of serum dexamethasone does not negatively affect the performance of the overnight low-dose DST (oDST)
- •
Reflex implementation greatly reduced the number of serum dexamethasone measurements thereby decreasing unnecessary costs
- •
The oDST appeared to be valid as long as there was a measurable serum dexamethasone result (>50 ng/dL)
Clinical Relevance
Introduction
Materials and Methods
Study Design
Study Population
Procedures
Data Collection
Outcomes Assessment
Statistical Analysis
Results
Study Population Characteristics

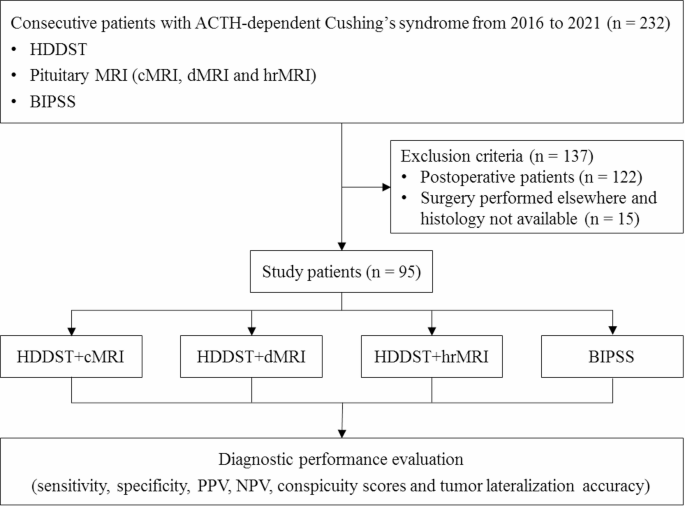
Figure 1. Flowchart of participants selection from 616 completed oDSTs completed 6 months before (n = 308) and after (n = 308) Reflex implementation. Subsequent oDSTs for the same patient and unmeasurable post-oDST serum dexamethasone (SerDex) (<50 ng/dL [Lower quantifiable limit]) were excluded from analysis. A total of 542 oDSTs were included for analysis and breakdown of CS diagnosis and etiology are shown. ACTH-dependent CS is further broken down to differentiate neoplastic (NH) versus non-neoplastic (NNH) etiologies. CS = Cushing Syndrome; NH = neoplastic hypercortisolism; NNH = nonneoplastic hypercortisolism; oDST = overnight dexamethasone suppression test; SerDex = serum dexamethasone.
Table 1. Demographic Characteristics of Patients Who Underwent oDST Before and After Reflex Implementation
| Empty Cell | Pre-Reflex | Post-Reflex | ||||
|---|---|---|---|---|---|---|
| Yes CS with NNH | Yes CS without NNH | No CS | Yes CS with NNH | Yes CS without NNH | No CS | |
| N | 38 | 34 | 223 | 40 | 38 | 241 |
| Age | ||||||
| Mean (SD) | 63.6 (13.8) | 63.8 (14.4) | 56.0 (15.1)a | 63.8 (13.2) | 63.1 (13.1) | 55.3 (15.5)b |
| Sex | ||||||
| Male (%) | 6 (15.8) | 4 (11.8) | 57 (25.6) | 11 (27.5) | 11 (28.9) | 67 (27.8) |
| Female (%) | 32 (84.2) | 30 (88.2) | 166 (74.4) | 29 (72.5) | 27 (71.1) | 174 (72.2) |
| Race | ||||||
| American Indian or Alaskan Native (%) | 0 | 0 | 1 (0.4) | 0 | 0 | 1 (0.4) |
| Asian (%) | 0 | 0 | 3 (1.3) | 0 | 0 | 1 (0.4) |
| Black or African American (%) | 5 (13.2) | 5 (14.7) | 27 (12.2) | 6 (15.0) | 6 (15.8) | 23 (9.5) |
| Other (%) | 2 (5.3) | 1 (2.9) | 8 (3.6) | 1 (2.5) | 1 (2.2) | 9 (3.8) |
| White (%) | 31 (81.5) | 28 (82.4) | 184 (82.5) | 33 (82.5) | 31 (82.0) | 207 (85.9) |
- a
-
Age different from group with CS within Pre-Reflex-oDST (P = 0.005).
- b
-
Age different from group with CS within Post-Reflex-oDST (P < 0.001) regardless of whether NNH cases are included. Male vs female distribution NS (χ2 = 2.533, 3 df, P = 0.469). Race distribution NS (χ2 = 4.37733, 12 df, P = 0.976).
Prereflex-oDST vs Post-reflex-oDST Analysis

Figure 2. Comparison of oDST serum cortisol (SerCort) levels Pre-vs Post-Reflex-oDST implementation. The medians are further stratified based on whether the patient did not have Cushing Syndrome (No CS – red) and those who had CS (Yes CS – blue). Each box represents the interquartile range and the horizontal line within represents the median. The error bars represent the 10th-90th percentiles and dots represent results outlying the 10th-90th percentiles. a, denotes significant difference of median SerCort levels between no CS vs CS in both Pre- and Post-Reflex-oDST groups (P < 0.001). There was no difference in medians following exclusion of NNH from Yes CS in both Pre- and Post-Reflex-oDST groups (P = 0.269). CS = Cushing Syndrome; NH = neoplastic hypercortisolism; NNH = nonneoplastic hypercortisolism; oDST = overnight dexamethasone suppression test; SerDex = serum dexamethasone.
Table 2. Receiver operating characteristic (ROC) analysis of oDST SerCort results for Pre-vs Post-Reflex-oDST groups. A. Analysis including NNH patients are at the top; B. Analysis excluding NNH patients are at the bottom
| Empty Cell | Pre-Reflex | Post-Reflex | ||||
|---|---|---|---|---|---|---|
| A. Including NNH patients | ||||||
| ROC Curve Area (SE) | 0.97 (0.01) | 0.97 (0.01) | ||||
| 95% confidence interval | 0.96-0.99 | 0.95-0.99 | ||||
| P value | P < 0.0001 | P < 0.0001 | ||||
| Sample size: No CS/Yes CS | 223/38 | 241/40 | ||||
| Cutoff | Sensitivity | Specificity | Cutoff | Sensitivity | Specificity | |
| Optimal 8 AM SerCort Cutoff (mcg/dL) | 2.1 | 92% | 93% | 2.1 | 95% | 93% |
| Empty Cell | Pre-Reflex without NNH | Post-Reflex without NNH | ||||
|---|---|---|---|---|---|---|
| B. Excluding NNH patients | ||||||
| ROC curve area (SE) | 0.97 (0.01) | 0.97 (0.01) | ||||
| 95% confidence interval | 0.96-0.99 | 0.95-0.99 | ||||
| P Value | P < 0.0001 | P < 0.0001 | ||||
| Sample size: No CS/Yes CS | 223/34 | 241/38 | ||||
| Cutoff | Sensitivity | Specificity | Cutoff | Sensitivity | Specificity | |
| Optimal 8 AM SerCort Cutoff (mcg/dL) | 2.1 | 91% | 92% | 2.1 | 95% | 93% |
Prereflex-oDST Comparison of SerDex vs SerCort

Figure 3. Comparison of post-oDST serum cortisol (SerCort) to serum dexamethasone (SerDex) in Pre-Reflex-oDST group. (A) Comparison of post-oDST SerCort and SerDex for no CS patients in the Pre-Reflex-oDST group. SerCort in the No CS patients stratified by the ARUP Lower limit of the reference range for SerDex (140 ng/dL). There was no significant difference in median SerCort with the SerDex <140 ng/dL (N = 20) and >140 ng/dL (N = 203) groups (1.2 vs 1.1 mcg/dL, respectively, P = 0.621). (B) Comparison of all Pre-Reflex-oDST group oDSTs stratified by patients with (blue) and without (red) CS. The black vertical solid line represents the limit of quantitation (LOQ) of SerDex (50 ng/dL). There was no correlation of SerDex and SerCort achieved in either group (see text for specifics). There was no correlation when NNH cases were removed as well (P = 0.432). CS = Cushing Syndrome; NH = neoplastic hypercortisolism; NNH = nonneoplastic hypercortisolism; oDST = overnight dexamethasone suppression test; SerDex = serum dexamethasone.
Discussion
Conclusion
Disclosure
Acknowledgment
References
- 1
H. Raff, T. CarrollCushing’s syndrome: from physiological principles to diagnosis and clinical careJ Physiol, 593 (3) (2015), pp. 493-506
- 2
J.W. Findling, H. RaffRecognition of nonneoplastic hypercortisolism in the evaluation of patients with cushing syndromeJ Endocr Soc, 7 (8) (2023), Article bvad087
- 3
J.W. Findling, H. RaffDiagnosis of endocrine disease: differentiation of pathologic/neoplastic hypercortisolism (Cushing’s syndrome) from physiologic/non-neoplastic hypercortisolism (formerly known as pseudo-cushing’s syndrome)Eur J Endocrinol, 176 (5) (2017), pp. R205-R216
- 4
M.S. Sagmeister, L. Harper, R.S. HardyCortisol excess in chronic kidney disease – a review of changes and impact on mortalityFront Endocrinol (Lausanne), 13 (2022), Article 1075809
- 5
R. Pivonello, A.M. Isidori, M.C. De Martino, J. Newell-Price, B.M. Biller, A. ColaoComplications of cushing’s syndrome: state of the artLancet Diabetes Endocrinol, 4 (7) (2016), pp. 611-629
- 6
M. Araujo-Castro, E. Pascual-Corrales, C. LamasPossible, probable, and certain hypercortisolism: a continuum in the risk of comorbidityAnn Endocrinol (Paris), 84 (2) (2023), pp. 272-284
- 7
M. Fassnacht, W. Arlt, I. Bancos, et al.Management of adrenal incidentalomas: European society of endocrinology clinical practice guideline in collaboration with the european network for the study of adrenal tumorsEur J Endocrinol, 175 (2) (2016), pp. G1-G34
- 8
M. Fleseriu, R. Auchus, I. Bancos, et al.Consensus on diagnosis and management of Cushing’s disease: a guideline updateLancet Diabetes Endocrinol, 9 (12) (2021), pp. 847-875
- 9
P.J. Wood, J.H. Barth, D.B. Freedman, L. Perry, B. SheridanEvidence for the low dose dexamethasone suppression test to screen for Cushing’s syndrome–recommendations for a protocol for biochemistry laboratoriesAnn Clin Biochem, 34 (Pt 3) (1997), pp. 222-229
- 10
L.K. Nieman, B.M. Biller, J.W. Findling, et al.The diagnosis of cushing’s syndrome: an endocrine society clinical practice guidelineJ Clin Endocrinol Metab, 93 (5) (2008), pp. 1526-1540
- 11
H. Raff, S.T. Sharma, L.K. NiemanPhysiological basis for the etiology, diagnosis, and treatment of adrenal disorders: cushing’s syndrome, adrenal insufficiency, and congenital adrenal hyperplasiaCompr Physiol, 4 (2) (2014), pp. 739-769
- 12
R.S. Mohamed, B. Abuelgasim, S. Barker, et al.Late-night salivary cortisol and cortisone should be the initial screening test for cushing’s syndromeEndocr Connect, 11 (7) (2022), Article e220050
- 13
S. GuthrieThe impact of dexamethasone pharmacokinetics on the DST: a reviewPsychopharmacol Bull, 27 (4) (1991), pp. 565-576
- 14
T. Nickelsen, W. Lissner, K. SchofflingThe dexamethasone suppression test and long-term contraceptive treatment: measurement of ACTH or salivary cortisol does not improve the reliability of the testExp Clin Endocrinol, 94 (3) (1989), pp. 275-280
- 15
A.W. MeikleDexamethasone suppression tests: usefulness of simultaneous measurement of plasma cortisol and dexamethasoneClin Endocrinol (Oxf), 16 (4) (1982), pp. 401-408
- 16
M. Fleseriu, A.H. Hamrahian, A.R. Hoffman, et al.American association of clinical endocrinologists and American college of endocrinology disease state clinical review: diagnosis of recurrence in cushing diseaseEndocr Pract, 22 (12) (2016), pp. 1436-1448
- 17
G.A. Ueland, P. Methlie, R. Kellmann, et al.Simultaneous assay of cortisol and dexamethasone improved diagnostic accuracy of the dexamethasone suppression testEur J Endocrinol, 176 (6) (2017), pp. 705-713
- 18
N. Genere, R.J. Kaur, S. Athimulam, et al.Interpretation of abnormal dexamethasone suppression test is enhanced with use of synchronous free cortisol assessmentJ Clin Endocrinol Metab, 107 (3) (2022), pp. e1221-e1230
- 19
B.R. Javorsky, H. Raff, T.B. Carroll, et al.New cutoffs for the biochemical diagnosis of adrenal insufficiency after ACTH stimulation using specific cortisol assaysJ Endocr Soc, 5 (4) (2021), Article bvab022
- 20
Centers for medicare & medicaid services – clinical laboratory fee scheduleAvailable from:https://www.cms.gov/medicare/payment/fee-schedules/clinical-laboratory-fee-schedule-clfs, Accessed 31st Jan 2025
- 21
A.H. Rosenbaum, A.F. Schatzberg, R.A. MacLaughlin, et al.The dexamethasone suppression test in normal control subjects: comparison of two assays and effect of ageAm J Psychiatry, 141 (12) (1984), pp. 1550-1555
- 22
S.M. RoperYield of serum dexamethasone measurement for reducing false-positive results of low-dose dexamethasone suppression testingJ Appl Lab Med, 6 (2) (2021), pp. 480-485
- 23
N. Vogg, M. Kurlbaum, T. Deutschbein, B. Grasl, M. Fassnacht, M. KroissMethod-specific cortisol and dexamethasone thresholds increase clinical specificity of the dexamethasone suppression test for cushing syndromeClin Chem, 67 (7) (2021), pp. 998-1007
- 24
D.G. Farinelli, K.C. Oliveira, L.F. Hayashi, C.E. KaterOvernight 1-mg dexamethasone suppression test for screening cushing syndrome and mild autonomous cortisol secretion (MACS): what happens when serum dexamethasone is below cutoff? How frequent is it?Endocr Pract, 29 (12) (2023), pp. 986-993
- 25
F. Ceccato, C. Artusi, M. Barbot, et al.Dexamethasone measurement during low-dose suppression test for suspected hypercortisolism: threshold development with and validationJ Endocrinol Invest, 43 (8) (2020), pp. 1105-1113
- 26
M. Keller-WoodHypothalamic-Pituitary–Adrenal axis-feedback controlCompr Physiol, 5 (3) (2015), pp. 1161-1182
- 27
E. Valassi, B. Swearingen, H. Lee, et al.Concomitant medication use can confound interpretation of the combined dexamethasone-corticotropin releasing hormone test in cushing’s syndromeJ Clin Endocrinol Metab, 94 (12) (2009), pp. 4851-4859
- 28
C.W. Wilkinson, E.R. Peskind, M.A. RaskindDecreased hypothalamic-pituitary-adrenal axis sensitivity to cortisol feedback inhibition in human agingNeuroendocrinology, 65 (1) (1997), pp. 79-90
Filed under: Cushing's, Diagnostic Testing | Tagged: ACTH, dexamethasone suppression test, endogenous, low-dose overnight serum dexamethasone suppression test, ODST | Leave a comment »


-circled-in-red")




{kind=link}
{kind=link}