Published online 2009 Jul 16. doi: 10.1055/s-0029-1220771
Hair Analysis Provides a Historical Record of Cortisol Levels in Cushing’s Syndrome
Abstract
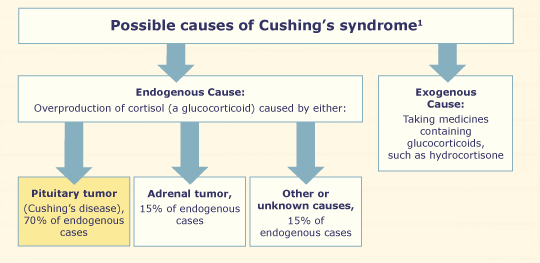
The severity of Cushing’s Syndrome (CS) depends on the duration and extent of the exposure to excess glucocorticoids. Current measurements of cortisol in serum, saliva and urine reflect systemic cortisol levels at the time of sample collection, but cannot assess past cortisol levels. Hair cortisol levels may be increased in patients with CS, and, as hair grows about 1 cm/month, measurement of hair cortisol may provide historical information on the development of hypercortisolism.
We attempted to measure cortisol in hair in relation to clinical course in six female patients with CS and in 32 healthy volunteers in 1 cm hair sections. Hair cortisol content was measured using a commercially available salivary cortisol immune assay with a protocol modified for use with hair.
Hair cortisol levels were higher in patients with CS than in controls, the medians (ranges) were 679 (279–2500) and 116 (26–204) ng/g respectively (P <0.001). Segmental hair analysis provided information for up to 18 months before time of sampling. Hair cortisol concentrations appeared to vary in accordance with the clinical course.
Based on these data, we suggest that hair cortisol measurement is a novel method for assessing dynamic systemic cortisol exposure and provides unique historical information on variation in cortisol, and that more research is required to fully understand the utility and limits of this technique.
Filed under: adrenal, Cushing's, pituitary | Tagged: abstract, Adrenal gland, Cancer, cortisol, Cushing's Syndrome, glucocorticoids, hair, hormones, Pituitary adenoma, saliva, serum, urine | Leave a comment »