Patients with different subtypes of Cushing’s syndrome (CS) have distinct plasma steroid profiles. This could be used as a test for diagnosis and classification, a German study says.
A quick diagnosis of CS is crucial so that doctors can promptly give therapy. However, diagnosing CS is often complicated by the multiple tests necessary not just to diagnose the disease but also to determine its particular subtype.
Cortisol, which leads to CS when produced at high levels, is a steroid hormone. But while earlier studies were conducted to determine whether patients with different subtypes of CS had distinct steroid profiles, the methods researchers used were cumbersome and have been discontinued for routine use.
Recently, a technique called LC-MS/MS has emerged for multi-steroid profiling in patients with adrenocortical dysfunction such as congenital adrenal hyperplasia, adrenal insufficiency and primary aldosteronism.
Researchers at Germany’s Technische Universität in Dresden used that method to determine whether patients with the three main subtypes of CS (pituitary, ectopic and adrenal) showed differences in plasma steroid profiles. They measured levels of 15 steroids produced by the adrenal glands in single plasma samples collected from 84 patients with confirmed CS and 227 age-matched controls.
They found that CS patients saw huge increases in the plasma steroid levels of 11-deoxycortisol (289%), 21-deoxycortisol (150%), 11-deoxycorticosterone (133%), corticosterone (124%) and cortisol (122%), compared to patients without the disease.
Patients with the ectopic subtype had the biggest jumps in levels of these steroids. However, plasma 18-oxocortisol levels were particularly low in ectopic disease. Other steroids demonstrated considerable variation.
Patients with the adrenal subtype had the lowest concentration of dehydroepiandrosterone (DHEA) and DHEA-SO4, which are androgens. Patients with the ectopic and pituitary subtype had the lowest concentration of aldosterone.
Through the use of 10 selected steroids, patients with different subtypes of CS could be identified almost as closely as with other tests, including the salivary and urinary free cortisol test, the dexamethasone-suppressed cortisol test, and plasma adrenocorticotropin levels. The misclassification rate using steroid levels was 9.5 percent, compared to 5.8 percent in other tests.
“This study using simultaneous LC-MS/MS measurements of 15 adrenal steroids in plasma establishes distinct steroid metabolome profiles that might be useful as a test for CS,” the team concluded, adding that using LC-MS/MS is advantageous, as specimen preparation is simple and the entire panel takes 12 minutes to run. This means it could be offered as a single test for both identification and subtype classification.
There is an increasing number of cases of aldosterone- and cortisol-producing adenomas (A/CPAs) reported in the context of primary aldosteronism (PA). Most of these patients have PA complicated with subclinical Cushing’s syndrome; cases of apparent Cushing’s syndrome (CS) complicated with aldosteronism are less reported. However, Co-secretory tumors were present in the right adrenal gland, a cortisol-secreting adenoma and an aldosterone-producing nodule (APN) were present in the left adrenal gland, and aldosterone-producing micronodules (APMs) were present in both adrenal glands, which has not been reported. Here, we report such a case, offering profound insight into the diversity of clinical and pathological features of this disease.
Case presentation
The case was a 45-year-old female from the adrenal disease diagnosis and treatment centre in West China Hospital of Sichuan University. The patient presented with hypertension, moon-shaped face, central obesity, fat accumulation on the back of the neck, disappearance of cortisol circadian rhythm, ACTH < 5 ng/L, failed elevated cortisol inhibition by dexamethasone, orthostatic aldosterone/renin activity > 30 (ng/dL)/(ng/mL/h), and plasma aldosterone concentration > 10 ng/dL after saline infusion testing. Based on the above, she was diagnosed with non-ACTH-dependent CS complicated with PA. Adrenal vein sampling showed no lateralization for cortisol and aldosterone secretion in the bilateral adrenal glands. The left adrenocortical adenoma was removed by robot-assisted laparoscopic resection. However, hypertension, fatigue and weight gain were not alleviated after surgery; additionally, purple striae appeared in the lower abdomen, groin area and inner thigh, accompanied by systemic joint pain. One month later, the right adrenocortical adenoma was also removed. CYP11B1 were expressed in the bilateral adrenocortical adenomas, and CYP11B2 was also expressed in the right adrenocortical adenomas. APN existed in the left adrenal gland and APMs in the adrenal cortex adjacent to bilateral adrenocortical adenomas. After another surgery, her serum cortisol and plasma aldosterone returned to normal ranges, except for slightly higher ACTH.
Conclusions
This case suggests that it is necessary to assess the presence of PA, even in CS with apparent symptoms. As patients with CS and PA may have more complicated adrenal lesions, more data are required for diagnosis.
Because both adrenal Cushing’s syndrome and primary aldosteronism (PA) can manifest as adrenocortical adenomas, it is difficult to distinguish between them on the sole basis of adrenal computed tomography (CT). There may also be multiple adenomas with different functions in the same adrenal gland [1], which also leads to the difficulty in the interpretation of adrenal vein blood collection results. With the increased reports on cases of PA complicated with subclinical Cushing’s syndrome in clinical practice, increasing attention is being given to the screening of PA complicated with subclinical Cushing’s syndrome. However, PA screening may be ignored in the diagnosis and treatment of adrenal Cushing’s syndrome.
Although it has been reported that PA with a diameter > 2 cm may be complicated with aldosterone- and cortisol-producing adenomas (A/CPAs) [2], cases of apparent Cushing’s syndrome complicated with PA are less well known.
Recently, Y. Fushimi et al. [3] reported a case of apparent Cushing’s syndrome complicated with PA. The cortisol-producing enzyme cytochrome P450 (CYP) 11B1 was diffusely expressed in the adenoma, but based on staining, the aldosterone synthase CYP11B2 was significantly expressed in the adjacent adrenal cortex. This finding indicated that aldosterone-producing micronodules (APMs) in the adjacent adrenal cortex may be the pathological basis of PA.
Here, a case of bilateral co-secretory lesions presenting with coexisting Cushing syndrome and primary aldosteronism detected by AVS and confirmed by immunohistochemical analysis after surgical resection is reported. Moreover, APMs were found in the adrenal cortex adjacent to bilateral adrenocortical adenomas; an aldosterone-producing nodule was detected adjacent to the unilateral adenoma.
Case presentation
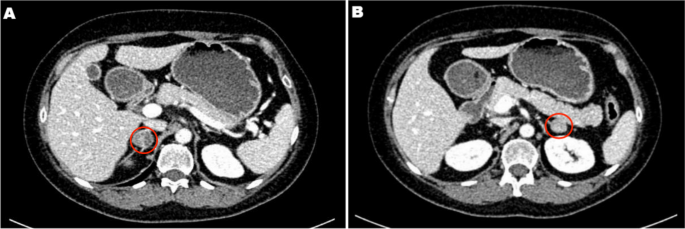
A 45-year-old female patient was admitted to the adrenal disease diagnosis and treatment centre in West China Hospital of Sichuan University due to “increased blood pressure, weight gain for one year and facial oedema for half a year”. After nifedipine controlled-release tablets 30 mg daily and terazosin 2 mg daily were applied, the blood pressure of this patient was still as high as 179/113 mmHg. She had no family history of endocrine disease or malignant tumour. Her body mass index (BMI) was 25.6 kg/m2 at admission, with a moon-shaped face, fat accumulation on the back of the neck and thin skin. Hormonal, glucose, renal function, lipid, and blood electrolyte tests were completed, and the physiological rhythm of cortisol had disappeared. Aldosterone-renin-angiotensin system (RAAS) results showed a significant decrease in renin activity and a significantly higher aldosterone/renin ratio (ARR) (as provided in Table 1). Dynamic testing for hormones was conducted, and the results were as follows: (i) in terms of the saline infusion test (SIT) in supine position, the before and after aldosterone level was 17.03 ng/dL and 15.45 ng/dL, respectively; (ii) in terms of the captopril challenge test (CCT), the before and after aldosterone level was 18.49 ng/dl and 15.25 ng/mL, respectively, with an inhibition rate of 17.52%; (iii) in terms of the standard low-dose dexamethasone suppression test, the before and after serum cortisol level was 467.9 nmol/L and 786.3 nmol/L, respectively; the before and after 24-h urine free cortisol (24-h UFC) level was 332.3 µg/24 and 480.4 µg/24, respectively. An enhanced CT scan revealed adenoma lesions in both adrenal glands (Fig. 1a and b). Bone mineral density measurement with dual-energy X-ray absorptiometry indicated osteoporosis. Chest CT showed old fractures of the 9th rib on the left side and the 2nd rib on the right side.
Table 1 Peripheral blood laboratory data for this case
Adrenal CT of the patient: A nodule with a size of approximately 1.6 × 1.5 cm was found in the left adrenal gland, and a nodule with a size of approximately 2.2 × 1.8 cm was found in the right adrenal gland. Irregular mild to moderate enhancement was on enhanced CT, and the surrounding fat gap was clear
Based on the above clinical features, the patient was diagnosed with “non-ACTH-dependent Cushing’s syndrome complicated with PA”. To assess lateralization, adrenal vein sampling (AVS) stimulated by ACTH was performed after obtaining informed consent. The results showed no lateralization of cortisol and aldosterone secretion (Table 2).
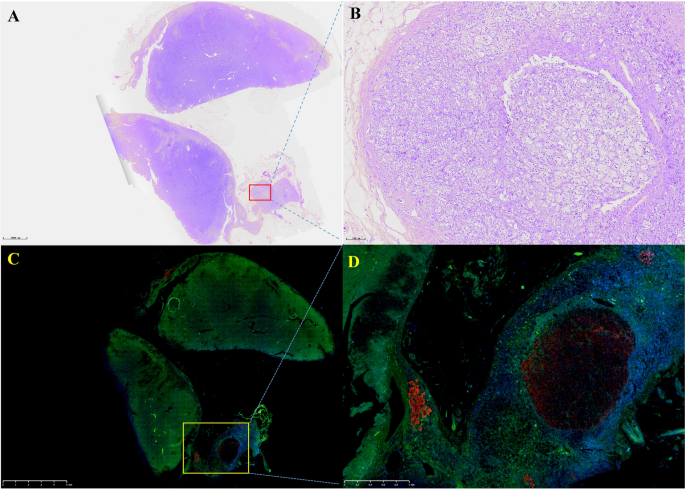
After communicating with the patient, the left adrenocortical adenoma was first removed by robot-assisted laparoscopic resection; the thickened adrenal cortex near the left adrenocortical adenoma was also resected during the surgery. The pathological report revealed adrenocortical adenoma, the Weiss score was 1, and immunohistochemistry showed weak CYP11B1 expression in the adenoma and positive CYP11B2 expression in an adjacent nodule. Hypertension was not alleviated after surgery. One month later, purple lines appeared on both sides of the lower abdomen, groin area and inner thigh, accompanied by weight gain, apparent systemic joint pain and fatigue in both lower limbs. The patient was readmitted to the hospital, and examination revealed orthostatic ALD at 11.99 ng/dL, PRA at 0.08 ng/mL/h, angiotensin II at 39.38 ng/L (reference range: 55.3–115.3 ng/L) and ARR at 149.88 (ng/dL)/(ng/mL/h). In addition, ACTH was 2.37 ng/L, serum cortisol was 352.30–353.50–283.90 nmol/L at 8 h-16 h-24 h, 24-h UFC was 112.8 µg, and serum cortisol was 342.10 nmol/L in the morning after the 1 mg dexamethasone suppression test. Enhanced CT of the kidneys and adrenal glands showed no solid nodules or masses in the left adrenal gland, though a nodule with a size of approximately 2.2*1.8 cm was detected in the right adrenal gland. Enhanced CT showed irregular mild to moderate enhancement. Therefore, the diagnosis was still “non-ACTH-dependent Cushing’s syndrome complicated with PA”. Subsequently, the right adrenocortical adenoma and the thickened adrenal cortex near the right adrenocortical adenoma were removed by robot-assisted laparoscopic resection. The pathological report indicated adrenocortical adenoma, and immunohistochemistry showed diffuse homogeneous expression of CYP11B1 and CYP11B2. Antibodies against CYP11B1 (MABS502) and CYP11B1 (MABS1251) were purchased from the Millipore Corporation. There were APMs in the adrenal cortex adjacent to the bilateral cortical adenomas. The fluorescence staining image of the left cortical adenoma is shown in Fig. 2. The immunohistochemistry image of the left adrenal gland is given in Fig. 3 and that of the right adrenal gland in Fig. 4. The immunofluorescence method used in this study was indirect immunofluorescence double staining procedure. Paraffin-embedded human adrenal tissues were prepared using heat-induced epitope retrieval after deparaffinization. Tissue sections were blocked with 5% goat serum in PBS, pH 7.4, containing 0.5% SDS, for 1 h. The slides were incubated with individual primary antibodies at 4℃ overnight, followed by incubation with Alexa Fluor 488-, and Alexa Fluor 647-conjugated secondary antibodies specific to the species of the primary antibodies with DAPI for immunofluorescence staining. Antibodies used included anti-CYP11B1 (Millipore, Cat. No. MABS502, 1:100), anti-CYP11B2(Millipore, Cat. No. MABS1251, 1:100), Alexa Fluor 488-conjugated anti-rat IgG secondary antibody (CYP11B1; Green) and Alexa Fluor 647-conjugated anti-mouse IgG secondary antibody (CYP11B2; Red). Nuclei were stained with DAPI.
Fig. 2
Routine hematoxylin and eosin (H&E) staining and immunofluorescence of the left adrenocortical adenoma (green represents expression of CYP11B1 and red that of CYP11B2). This adrenocortical adenoma and the surrounding cortex was cut into three parts. A and C show the overall appearance of the resected portion, with a nodule adjacent to the adenoma. B shows a neoplastic lesion formed by clear cells (aldosterone-producing cell) within nodules, lacking a fibrous envelope. C clearly shows the weak and diffuse expression of CYP11B1 in adrenocortical adenoma and CYP11B2 expression in a nodule in the cortex adjacent to the adenoma. D shows local enlargement of the aldosterone-producing nodule and three aldosterone-producing micronodules adjacent to it
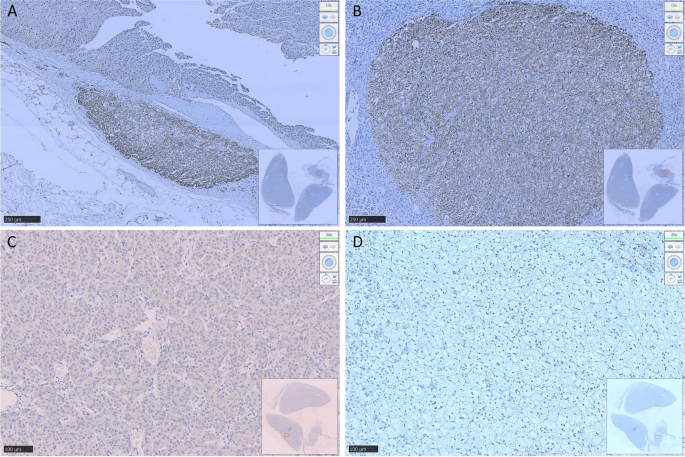
Resected adrenocortical adenoma and part of the adrenal cortex on the left side. A shows expression of Aldosterone-producing micronodule CYP11B2 in the cortex adjacent to the adenoma. B shows an aldosterone-producing nodule with a diameter of approximately 2 mm. C shows weak positive expression of CYP11B1 in the adenoma and D negative expression of CYP11B1 in the aldosterone-producing nodule
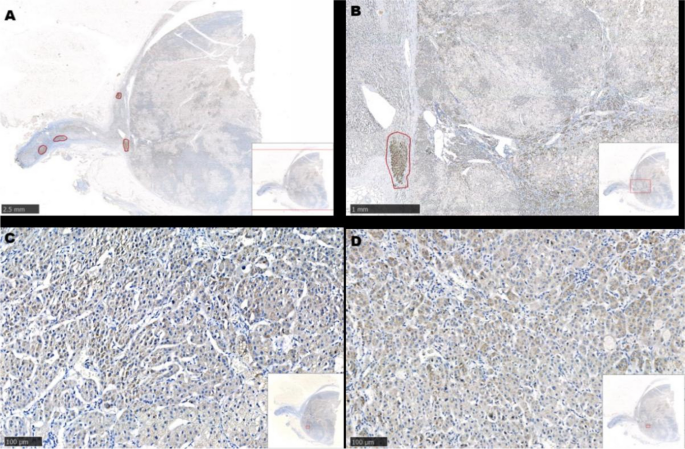
Resected adrenocortical adenoma and part of the adrenal cortex on the right side. A and B show several Aldosterone-producing micronodules (positive expression of CYP11B2) in the cortex adjacent to the adenoma. C shows diffuse expression of CYP11B1 in the adenoma. D shows diffuse expression of CYP11B2 in the adenoma
The Cushing’s syndrome in this patient disappeared after surgery, and glucocorticoids were discontinued after 15 months according to medical advice. Follow-up was conducted for half a year after drug discontinuance, and the patient had no fatigue or dizziness; she was satisfied with the outcomes. Her systolic and diastolic blood pressure remained at 100–120 mmHg and 70–80 mmHg, respectively. During the most recent re-examination, the following results were obtained: (1) orthostatic ALD of 19.1 ng/dL and orthostatic renin concentration of 12.59 µIU/mL, with an aldosterone/renin ratio (ARR) of 1.52; (2) PTC at 8 AM of 247 nmol/L, ACTH of 93.55 ng/L and 24-h UFC of 26.8 µg; (3) parathyroid hormone of 3.86 pmol/L; (4) 25-OH-VitD of 119.5 nmol/L; (5) serum creatinine of 60 µmol/L; (6) serum sodium of 140.4 nmol/L, serum potassium of 3.87 mmol/L and serum calcium of 2.27 mmol/L.
Discussion and conclusions
Adrenal Cushing’s syndrome is caused by excessive autonomic secretion of cortisol induced by adrenal cortical tumours or adrenal cortical hyperplasia; primary aldosteronism (PA) is caused by excessive autonomic secretion of aldosterone induced by adrenal cortical tumours or adrenal cortical hyperplasia. More adverse symptoms occur if aldosterone and cortisol-producing adenomas are present. Specifically, (1) it is more difficult to control hypertension; (2) the incidence of major adverse cardiovascular and cerebrovascular events would increase [4]; (3) glucose intolerance and other metabolic complications would be aggravated [5, 6]; (4) patients would be prone towards osteoporosis [7, 8]; (5) adrenal vein sampling results may be misinterpreted [9]; and (6) adrenal insufficiency may occur after surgery. Therefore, it is of great clinical significance to avoid missed diagnosis of A/CPAs.
Despite many reports on A/CPAs, the majority of these patients may have subclinical Cushing’s syndrome (SCS), and cases of apparent Cushing’s syndrome complicated with PA are rarely reported. In the present case, the clinical manifestation of Cushing’s syndrome were more apparent, and it would be appropriate to call it cortisol-aldosterone cosecretoma. Naoyoshi Onoda et al. [10] reported a case of Cushing’s syndrome caused by a left adrenocortical adenoma (30 mm in diameter) and PA caused by a right adrenocortical adenoma (20 mm in diameter), and Fushimi et al. [3] reported a case of right A/CPA (25 mm*22 mm in size). Interestingly, in the present report, the patient had bilateral A/CPAs, and the clinical manifestations of Cushing’s syndrome became more apparent after unilateral resection was performed. Similar to the above two cases, APMs were found in the adrenal cortex adjacent to the A/CPAs, but aldosterone-producing nodules were found near the cortisol-producing adenoma on the left side.
The biochemical phenotype of APM-inducing autonomic aldosterone secretion has not been clarified. APMs can also be found in the adrenal tissue of 30% of individuals with normal blood pressure [11] and surrounding areas of APA [12, 13]. APMs do not express CYP11B1 or CYP17A1, which are necessary for the generation of cortisol [12, 14]. In our patient, the aldosterone-producing nodule in the left adrenal gland may have developed from APM. More than one-third of APMs carry known mutations in CACNA1D and ATP1A1, promoting the generation of aldosterone [14, 15]. Unfortunately, we did not perform whole-exome sequencing on the DNA of the peripheral blood and adenoma tissues of this patient. Due to the existence of APMs adjacent to the adenoma, it remains unclear whether there is a risk of the relapse of PA in these cases after resection of adrenal the adenoma. Therefore, it was necessary to conduct medical follow-up for this patient.
Remi Goupil et al. performed AVS on 8 patients with cortisol-producing adenoma (CPA), and the results showed that cortisol on the CPA side was higher than that on the contralateral side (median, 6.7 times [range: 2.4–27.2]); P = 0.012]) [16]. There was no significant difference in bilateral cortisol and aldosterone concentrations after AVS in this patient, which is consistent with bilateral A/CPA. Although immunohistochemical results revealed weak expression of CYP11B1 for the first time, expression of cortisol in bilateral adrenal venous blood samples increased significantly after ACTH stimulation. Hence, cortisol was over-synthesized on both sides, and bilateral A/CPAs was definitively diagnosed.
In summary, this case highlights the need for A/CPA screening. The complicated pathological features of these cases impose challenges to our understanding of this disease. Due to the presence of APMs in the adrenal cortex near bilateral adrenocortical adenomas, more clinical data are required to identify whether the disease might relapse after simple resection of the adenoma in these patients. Therefore, further medical follow-up of these patient is needed.
Availability of data and materials
Not applicable.
Abbreviations
CS:
Cushing’s syndrome
PA:
Primary aldosteronism
ACTH:
Adrenocorticotropic hormone
UFC:
Urinary free cortisol
AVS:
Adrenal vein sampling
A/CPA:
Aldosterone-and cortisol producing adenoma
APN:
Aldosterone-producing nodules
APM:
Aldosterone-producing micronodule
CYP:
Cytochrome P450
CT:
Computed tomography
PAC:
Plasma aldosterone concentration
PRA:
Plasma renin activity
ARR:
Aldosterone /renin ratio
References
Stenman A, Shabo I, Ramström A, Zedenius J, Juhlin CC: Synchronous aldosterone- and cortisol-producing adrenocortical adenomas diagnosed using CYP11B immunohistochemistry. SAGE open medical case reports. 2019, 7:2050313×19883770.
Hiraishi K, Yoshimoto T, Tsuchiya K, Minami I, Doi M, Izumiyama H, Sasano H, Hirata YJ. Clinicopathological features of primary aldosteronism associated with subclinical Cushing’s syndrome. Endocr J. 2011;58(7):543–51.
Fushimi Y, Tatsumi F, Sanada J, Shimoda M, Kamei S, Nakanishi S, Kaku K, Mune T, Kaneto H. Concurrence of overt Cushing’s syndrome and primary aldosteronism accompanied by aldosterone-producing cell cluster in adjacent adrenal cortex: case report. BMC Endocr Disord. 2021;21(1):163.
Araujo-Castro M, BengoaRojano N, FernándezArgüeso M, Pascual-Corrales E, Jiménez Mendiguchía L. García Cano AMCardiometabolic risk in patients with primary aldosteronism and autonomous cortisol secretion. Case-control study. Med Clin (Barc). 2021;157(10):473–9.
Petramala L, Olmati F, Concistrè A, Russo R, Mezzadri M, Soldini M, De Vincentis G, Iannucci G, De Toma G, Letizia C. Cardiovascular and metabolic risk factors in patients with subclinical Cushing. Endocrine. 2020;70(1):150–63.
Akehi Y, Yanase T, Motonaga R, Umakoshi H, Tsuiki M, Takeda Y, Yoneda T, Kurihara I, Itoh H, Katabami T, et al. High Prevalence of Diabetes in Patients With Primary Aldosteronism (PA) Associated With Subclinical Hypercortisolism and Prediabetes More Prevalent in Bilateral Than Unilateral PA: A Large Multicenter Cohort Study in Japan. Diabetes Care. 2019;42(5):938–45.
Shi S, Lu C, Tian H, Ren Y, Chen T. Primary Aldosteronism and Bone Metabolism: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne). 2020;11:574151.
Petramala L, Zinnamosca L, Settevendemmie A, Marinelli C, Nardi M, Concistrè A, Corpaci F, Tonnarini G, De Toma G, Letizia C. Bone and mineral metabolism in patients with primary aldosteronism. Int J Endocrinol. 2014;2014:836529.
Späth M, Korovkin S, Antke C, Anlauf M, Willenberg HS. Aldosterone- and cortisol-co-secreting adrenal tumors: the lost subtype of primary aldosteronism. Eur J Endocrinol. 2011;164(4):447–55.
Onoda N, Ishikawa T, Nishio K, Tahara H, Inaba M, Wakasa K, Sumi T, Yamazaki T, Shigematsu K, Hirakawa K. Cushing’s syndrome by left adrenocortical adenoma synchronously associated with primary aldosteronism by right adrenocortical adenoma: report of a case. Endocr J. 2009;56(3):495–502.
Williams T, Gomez-Sanchez C, Rainey W, Giordano T, Lam A, Marker A, Mete O, Yamazaki Y, Zerbini M, Beuschlein F, et al. International Histopathology Consensus for Unilateral Primary Aldosteronism. J Clin Endocrinol Metab. 2021;106(1):42–54.
Nishimoto K, Tomlins SA, Kuick R, Cani AK, Giordano TJ, Hovelson DH, Liu CJ, Sanjanwala AR, Edwards MA, Gomez-Sanchez CE, et al. Aldosterone-stimulating somatic gene mutations are common in normal adrenal glands. Proc Natl Acad Sci U S A. 2015;112(33):E4591-4599.
Omata K, Anand SK, Hovelson DH, Liu CJ, Yamazaki Y, Nakamura Y, Ito S, Satoh F, Sasano H, Rainey WE, et al. Aldosterone-producing cell clusters frequently harbor somatic mutations and accumulate with age in normal adrenals. J Endocr Soc. 2017;1(7):787–99.
Lalli E, Barhanin J, Zennaro MC, Warth R. Local Control of Aldosterone Production and Primary Aldosteronism. Trends Endocrinol Metab. 2016;27(3):123–31.
Goupil R, Wolley M, Ahmed AH, Gordon RD, Stowasser M. Does concomitant autonomous adrenal cortisol overproduction have the potential to confound the interpretation of adrenal venous sampling in primary aldosteronism? Clin Endocrinol (Oxf). 2015;83(4):456–61.
This study was supported by the Discipline Excellence Development 1.3.5 Project of West China Hospital, Sichuan University (No. ZYGD18022).
Author information
Authors and Affiliations
Department of Endocrinology and Metabolism, Adrenal Center, West China Hospital of Sichuan University, Chengdu, 610041, Sichuan, ChinaHongjiao Gao, Yan Ren, Tao Chen & Haoming Tian
Department of Endocrinology and Metabolism, The Third Affiliated Hospital of Zunyi Medical University (The First People’s Hospital of Zunyi), Zunyi, Guizhou, ChinaHongjiao Gao
Institute of Clinical Pathology, West China Hospital of Sichuan University, Chengdu, Sichuan, ChinaLi Li & Fei Chen
Contributions
HG, TC researched data and/or wrote the manuscript. LL, FC contributed to immumohistochemical staining. HT, TC, YR contributed to discussion. All authors have read and approved the manuscript.
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
We do not have any potential conflicts of interest relevant to this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Gao, H., Li, L., Chen, F. et al. Bilateral co-secretory lesions presenting with coexisting Cushing syndrome and primary aldosteronism: a case report. BMC Endocr Disord23, 263 (2023). https://doi.org/10.1186/s12902-023-01454-8
The diagnosis of Cushing’s syndrome is challenging; however, through the clinical picture and the search for secondary causes of osteoporosis, it was possible to reach the diagnosis of the case reported. There was an independent, symptomatic ACTH hypercortisolism manifested by typical phenotypic changes, severe secondary osteoporosis and arterial hypertension in a young patient.
Case presentation
A 20-year-old Brazilian man with low back pain for 8 months. Radiographs showed fragility fractures in the thoracolumbar spine, and bone densitometry showed osteoporosis, especially when evaluating the Z Score (− 5.6 in the lumbar spine). On physical examination, there were wide violaceous streaks on the upper limbs and abdomen, plethora and fat increase in the temporal facial region, hump, ecchymosis on limbs, hypotrophy of arms and thighs, central obesity and kyphoscoliosis. His blood pressure was 150 × 90 mmHg. Cortisol after 1 mg of dexamethasone (24.1 µg/dL) and after Liddle 1 (28 µg/dL) were not suppressed, despite normal cortisoluria. Tomography showed bilateral adrenal nodules with more severe characteristics. Unfortunately, through the catheterization of adrenal veins, it was not possible to differentiate the nodules due to the achievement of cortisol levels that exceeded the upper limit of the dilution method. Among the hypotheses for the differential diagnosis of bilateral adrenal hyperplasia are primary bilateral macronodular adrenal hyperplasia, McCune–Albright syndrome and isolated bilateral primary pigmented nodular hyperplasia or associated with Carney’s complex. In this case, primary pigmented nodular hyperplasia or carcinoma became important etiological hypotheses when comparing the epidemiology in a young man and the clinical-laboratory-imaging findings of the differential diagnoses. After 6 months of drug inhibition of steroidogenesis, blood pressure control and anti-osteoporotic therapy, the levels and deleterious metabolic effects of hypercortisolism, which could also impair adrenalectomy in the short and long term, were reduced. Left adrenalectomy was chosen, given the possibility of malignancy in a young patient and to avoid unnecessary definitive surgical adrenal insufficiency if the adrenalectomy was bilateral. Anatomopathology of the left gland revealed expansion of the zona fasciculate with multiple nonencapsulated nodules.
Conclusion
The early identification of Cushing’s syndrome, with measures based on the assessment of risks and benefits, remains the best way to prevent its progression and reduce the morbidity of the condition. Despite the unavailability of genetic analysis for a precise etiological definition, it is possible to take efficient measures to avoid future damage.
Cushing’s syndrome may be exogenous or endogenous and, in this case, can be ACTH-dependent or independent. In the case reported, there was an independent, symptomatic ACTH hypercortisolism manifested by typical phenotypic changes, severe secondary osteoporosis and arterial hypertension in a young patient. Osteoporosis secondary to hypercortisolism occurs due to chronic reduction in bone formation, loss of osteocytes and increased reabsorption caused by intense binding of cortisol to glucocorticoid receptors present in bone cells [1]. In addition, excess cortisol impairs vitamin D metabolism and reduces endogenous parathyroid hormone secretion, intestinal calcium reabsorption, growth hormone release, and lean body mass [2]. Subclinical Cushing disease occurs in up to 11% of individuals diagnosed with early-onset osteoporosis and 0.5–1% of hypertension patients. [3] A cross-sectional study published in 2023 revealed a prevalence of 81.5% bone loss in 19 patients with Cushing’s syndrome [2]. The prevalence of osteopenia ranges from 60 to 80%, and the prevalence of osteoporosis ranges from 30 to 65% in patients with Cushing’s syndrome. Additionally, the incidence of fragility fractures ranges from 30 to 50% in these patients [4] and is considered the main cause of morbidity affecting the quality of life. The diagnosis is challenging, given the presence of confounding factors; however, through the clinical picture and the search for secondary causes of osteoporosis, it was possible to reach a syndromic diagnosis. Early identification of this syndrome, with measures based on the assessment of risks and benefits, remains the best way to prevent progression and reduce morbidity related to this disease [2].
Case presentation
A 20-year-old Brazilian male patient reported low back pain that had evolved for 8 months, with no related trauma. He sought emergency care and performed spinal radiographs on this occasion (03/2019). Due to the several alterations observed in the images, he was referred to the Orthopedics Service of the Hospital of Federal University of Juiz de Fora, which prescribed orthopedic braces, indicated physical therapy and was referred again to the Osteometabolic Diseases outpatient clinic of the Endocrinology and Rheumatology Services of the Hospital of Federal University of Juiz de Fora on 10/2019.
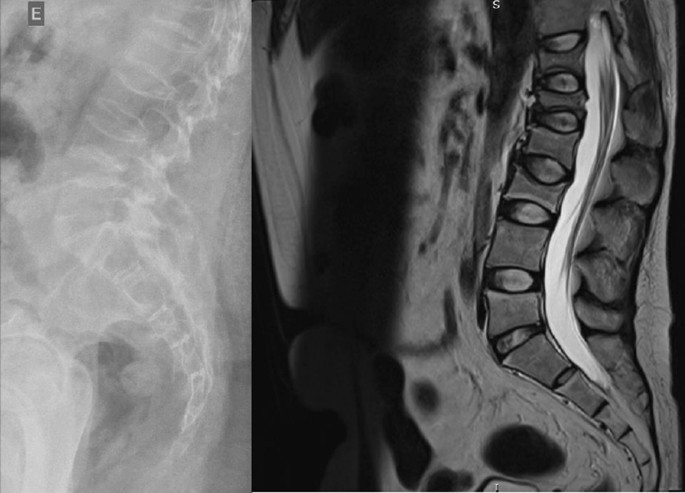
The radiographs showed a marked reduction in the density of bone structures, scoliotic deviation with convexity toward the left and reduction in the height of the lumbar vertebrae, with partial collapses of the vertebral bodies at the level of T12, L1, L2, L3 and L5, with recent collapses in T12 and L1, suggesting bone fragility fractures. The same can be seen in posterior magnetic resonance imaging (Fig. 1).
Fig. 1
Radiography and Magnetic Resonance Imaging (MRI) of lumbosacral spine in profile
Bone scintigraphy on 08/2019 did not reveal hyper flow or anomalous hyperemia in the topography of the thoracolumbar spine, and in the later images of the exam, there was a greater relative uptake of the tracer in the lumbar spine (vertebrae T10–T12, L2–L4), of nonspecific aspect, questioning the presence of osteoarticular processes or ankylosing spondylitis.
It was also observed in the bone densitometry requested in October 2019, performed by dual-energy X-ray absorptiometry (DXA), low bone mineral density (BMD) in the lumbar spine, femoral neck and total femur, when comparing the results to evaluating the Z Score (Table 1).
Thus, the diagnosis of osteoporosis was established, and treatment with vitamin D 7000 IU per week was started due to vitamin D3 insufficiency associated with the bisphosphonate alendronate 70 mg, also weekly. The patient had a past pathological history of fully treated syphilis (2018) and perianal condyloma with a surgical resection on 09/2017 and 02/2018. In the family history, it was reported that a maternal uncle died of systemic sclerosis. In the social context, the young person denied drinking alcohol and previous or current smoking.
On physical examination, there were no lentiginous skin areas or blue nevi; however, wide violet streaks were observed on the upper limbs and abdomen, with plethora and increased fat in the temporal facial region and hump (Fig. 2a, b), limb ecchymosis, hypotrophy of the arms and thighs, central obesity and kyphoscoliosis. Systemic blood pressure (sitting) was 150 × 90 mmHg, BMI was 26.09 kg/m2, and waist circumference was 99 cm, with no reported reduction in height, maintained at 1.55 m.
Fig. 2
Changes in the physical examination. a Violet streaks on the upper limbs, b Violet streaks on abdomen
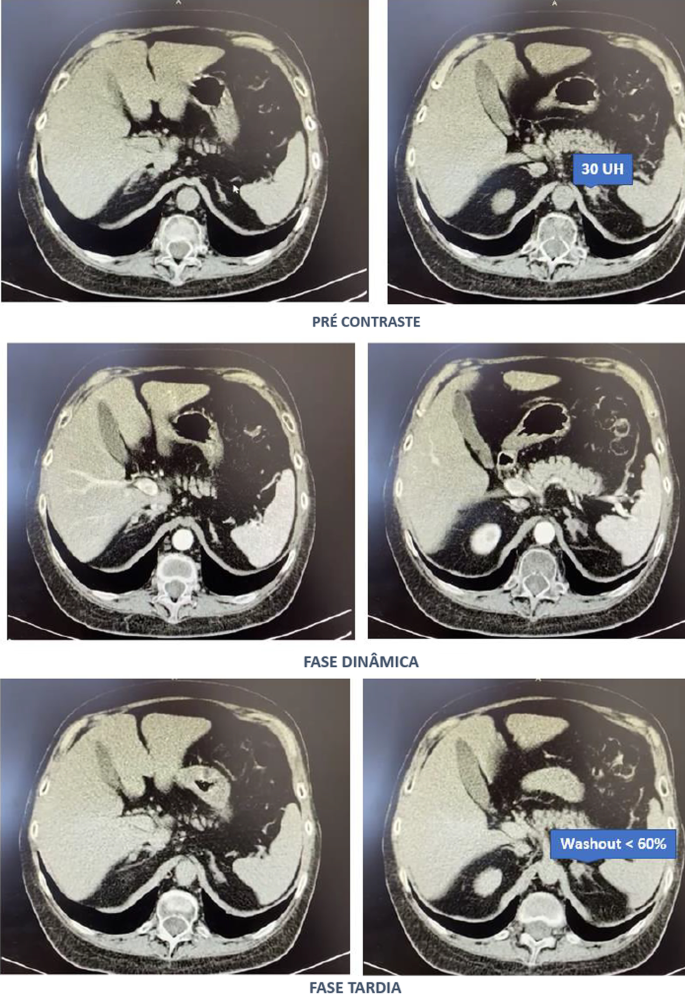
Computed tomography of the abdomen with adrenal protocol performed on 08/13/2020 characterized isodense nodular formation in the body of the left adrenal and in the lateral portion of the right adrenal, measuring 1.5 cm and 0.6 cm, respectively. The lesions had attenuation of approximately 30 HU, showing enhancement by intravenous contrast, with an indeterminate washout pattern in the late phase after contrast (< 60%) (Fig. 3).
After contact with the interventional radiology of the Hospital of Federal University of Juiz de Fora, catheterization of adrenal veins was performed on 10/2020; however, it was not possible to perform adequate lesion characterization due to obtaining serum cortisol levels that extrapolated the dilutional upper limit of the method (Table 3).
The calculation of the selectivity index was 6.63 (Reference Value (RV) > 3), confirming the good positioning of the catheter within the vessels during the procedure. The calculated lateralization index was 1.1296 (VR < 3), denoting bilateral hormone production. However, as aldosterone was not collected from a peripheral vein, it was not possible to obtain the contralateral rate and define whether there was contralateral suppression of aldosterone production [5].
Due to pending diagnoses for a better therapeutic decision and Cushing’s syndrome in clear evolution and causing organic damage, it was decided, after catheterization, to make changes in the patient’s drug prescription. Ketoconazole 400 mg per day was started, the dose of vitamin D was increased to 14,000 IU per week, and ramipril 5 mg per day was prescribed due to secondary hypertension. In addition, given the severity of osteoporosis, it was decided to replace previously prescribed alendronate with zoledronic acid.
Magnetic resonance imaging of the upper abdomen was performed on 06/19/2021, which demonstrated lobulated nodular thickening in the left adrenal gland with areas of decreased signal intensity in the T1 out-phase sequence, denoting the presence of fat, and homogeneous enhancement using contrast, measuring approximately 1.7 × 1.5 × 1.3 cm, suggestive of an adenoma. There was also a small nodular thickening in the lateral arm of the right adrenal, measuring approximately 0.8 × 0.6 cm, which was difficult to characterize due to its small dimensions and nonspecific appearance.
PPNAD or carcinoma became an important etiological hypothesis for the case described when comparing the epidemiology in a young man and the clinical-laboratory-imaging findings of the differential diagnoses. According to a dialog with the patient and family, the group of experts opted for unilateral glandular surgical resection on the left side (11/11/2021), where more significant changes were visualized, as there was a possibility of malignancy in a young patient and to avoid a definitive adrenal insufficiency condition because of bilateral adrenalectomy. This would first allow the analysis of the material and follow-up of the evolution of the condition with the permanence of the contralateral gland.
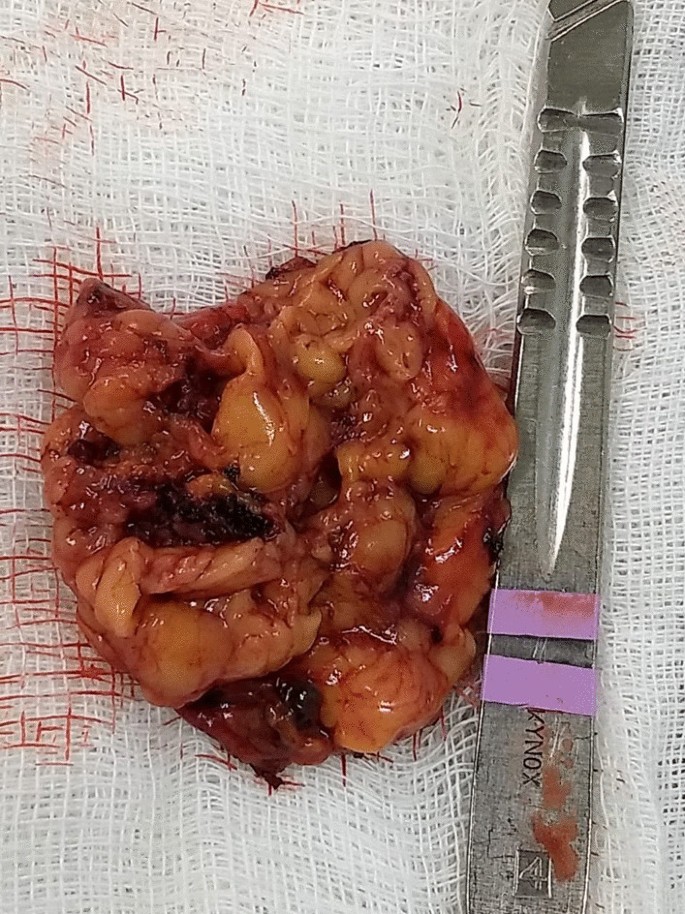
In the macroscopic analysis of the adrenalectomy specimen, adrenal tissue weighing 20 g and measuring 9.3 × 5.5 × 2.0 cm was described, completely surrounded by adipose tissue. The gland has a multinodular surface and varies between 0.2 and 1.6 cm in thickness, showing a cortex of 0.1 cm in thickness and a medulla of 1.5 cm in thickness (Fig. 4).
The microscopic analysis described the expansion of the zona fasciculate, with the formation of multiple nonencapsulated nodules composed of polygonal cells with ample and eosinophilic cytoplasm and frequent depletion of intracytoplasmic lipid content. No areas of necrosis or mitotic activity were observed. The histopathological picture is suggestive of cortical pigmented micronodular hyperplasia of the adrenal gland.
For the final etiological definition and an indication of contralateral adrenalectomy, which could be unnecessary and would avoid chronic corticosteroid therapy, or else, it would be necessary to protect the patient from future complications with the maintenance of the disease in the right adrenal gland, it would be essential to search for mutations in the PRKAR1A, PDE11A, PDE8B and PRKACA genes [15]; however, such genetic analysis is not yet widely available, and the impossibility of carrying it out at the local level did not allow a complete conclusion of the case.
Discussion
Through the clinical picture presented and the research of several secondary causes for osteoporosis, it was possible to arrive at the diagnosis of Cushing syndrome [6]. There was symptomatic independent ACTH hypercortisolism, manifested by typical phenotypic changes, severe secondary osteoporosis, and arterial hypertension in a young patient.
The diagnosis of Cushing’s syndrome is always challenging, given the presence of confounding factors such as the following:
Frequent and, even unknown, short- and long-term use of corticosteroids under different presentations;
Increase in the general population incidence of diabetes and obesity;
Screening tests with singularities for collection and individualized for different patient profiles.
It is important to note that the basal morning cortisol measurement is not the ideal test to assess hypercortisolism and is better applied to the assessment of adrenal insufficiency. However, the hypercortisolism of the case was unequivocal, and this test was also shown to be altered several times. As no test is 100% accurate, the current guidelines suggest the use of at least two first-line functional tests that focus on different aspects of the pathophysiology of the hypothalamic‒pituitary‒adrenal axis to confirm the hypercortisolism state: 24-hours cortisol, nocturnal salivary cortisol, morning serum cortisol after suppression with 1 mg of dexamethasone or after Liddle 1. Given that night-time salivary cortisol would require hospitalization, the other suggested tests were chosen, which are easier to perform in this context [7, 8].
Subsequently, tests were performed to determine the cause of hypercortisolism, such as serum ACTH levels and adrenal CT. The suppressed ACTH denoted the independence of its action. CT showed bilateral adrenal nodules with more severe features: solid lesion, attenuation > 10 UI on noncontrast images, and contrast washout speed < 60% in 10 minutes. In this case, it is essential to make a broad clinical decision and dialog with the patient to weigh and understand the risks and benefits of surgical treatment [9].
Among the main diagnostic hypotheses for the differential diagnosis of bilateral adrenal hyperplasia are primary bilateral macronodular adrenal hyperplasia, McCune–Albright syndrome (MAS) and bilateral primary pigmented nodular hyperplasia (PPNAD) isolated or associated with Carney’s complex. Another possibility would be bilateral adrenocorticotropic hormone (ACTH)-dependent macronodular hyperplasia secondary to long-term adrenal stimulation in patients with Cushing’s disease (ACTH-secreting pituitary tumor) or ectopic ACTH production, but the present case did not present with ACTH elevation.
Primary macronodular adrenal hyperplasia (nodules > 1 cm) predominates in women aged 50–60 years and may also be detected in early childhood (before 5 years) in the context of McCune–Albright syndrome. Most cases are considered sporadic; however, there are now several reports of familial cases whose presentation suggests autosomal dominant transmission. Several pathogenic molecular causes were identified in the table, indicating that it is a heterogeneous disease [10]. The pathophysiology occurs through the expression of anomalous ectopic hormone receptors or amplified eutopic receptors in the adrenals. It usually manifests in an insidious and subclinical way, with cortisol secretion mediated through receptors for gastric inhibitory peptide (GIP), vasopressin (ADH), catecholamines, interleukin 1 (IL-1), leptin, luteinizing hormone (LH), serotonin or others. Nodular development is not always synchronous or multiple; thus, hypercortisolism only manifests when there is a considerable increase in the number of adrenocortical cells, with severe steroidogenesis observed by cortisoluria greater than 3 times the upper limit of normal. Patients with mild Cushing’s syndrome should undergo screening protocols to identify aberrant receptors, as this may alter the therapeutic strategy. If there is evidence of abnormal receptors, treatment with beta-blockers is suggested for patients with beta-adrenergic receptors or with gonadotropin-releasing hormone (GnRH) agonists (and sex steroid replacement) for patients with LH/hCG receptors. In patients in whom aberrant hormone receptors are not present or for whom no specific pharmacological blockade is available or effective, the definitive treatment is bilateral adrenalectomy, which is known to make the patient dependent on chronic corticosteroid therapy [11]. Studies have shown the effectiveness of unilateral surgery in the medium and long term, opting for the resection of the adrenal gland of greater volume and nodularity by CT, regardless of the values obtained by catheterization of adrenal veins, but with the possibility of persistence or recurrence in the contralateral gland. Another possibility would be total unilateral adrenalectomy associated with subtotal contralateral adrenalectomy [12].
In McCune–Albright syndrome (MAS), there are activating mutations in the G-protein GNAS1 gene, generating autonomic hyperfunction of several tissues, endocrine or not, and there may be, for example, a constant stimulus similar to ACTH on the adrenal gland. In this case, pituitary levels of ACTH are suppressed, and adrenal adenomas with Cushing’s syndrome appear. Hypercortisolism may occur as an isolated manifestation of the syndrome or be associated with the triad composed of polyostotic fibrous dysplasia, café au lait spots with irregular borders and gonadal hyperfunction with peripheral precocious puberty. The natural history of Cushing’s syndrome in McCune-Albright syndrome (MAS) is heterogeneous, with some children evolving with spontaneous resolution of hypercortisolism, while others have a more severe condition, eventually requiring bilateral adrenalectomy [13].
PPNAD predominates in females, in people younger than 30 years, multiple and small (< 6 mm) bilateral pigmented nodules (surrounded by atrophied cortex), which can reach 1.5 cm in adulthood, with family genetic inheritance (66%) or sporadic inheritance (33%), and as part of the Carney complex reported in 40% of cases. In 70% of cases, inactivating mutations are identified in the PKA regulatory 1-alpha subunit (PRKAR1A), a tumor suppressor gene [14]. Osteoporosis is often associated with this condition [15]. One test that can distinguish patients with PPNAD from other primary adrenocortical lesions is cortisoluria after sequential suppression with low- and high-dose dexamethasone. In contrast to most patients with primary adrenocortical disease, who demonstrate no change in urinary cortisol, 70% of PPNAD patients have a paradoxical increase in urinary cortisol excretion [16]. The treatment of choice for PPNAD is bilateral adrenalectomy due to the high recurrence rate for primary adrenal disease [17].
Carney complex is a multiple neoplastic syndrome with autosomal dominant transmission, characterized by freckle-like cutaneous hyperpigmentation (lentiginosis), endocrine tumors [(PPNAD), testicular and/or thyroid tumors and acromegaly] and nonendocrine tumors, including cutaneous, cardiac, mammary, and osteochondral myxomas, among others. In the above case, the transthoracic echocardiogram of the patient on 03/18/2021 showed cavities of normal dimensions, preserved systolic and diastolic functions, no valve changes and no lentiginous skin areas and blue nevi, making the diagnosis of the syndrome less likely. The definitive diagnosis of Carney requires two or more main manifestations. Several related clinical components may suggest the diagnosis but not define it. The diagnosis can also be made if a key criterion is present and a first-degree relative has Carney or an inactivating mutation of the gene encoding PRKAR1A [18].
The adenoma is usually small in size (< 3 cm), similar to the nodules in this case; however, it is usually unilateral, with an insidious and mild evolution, especially in adult women over 35 years of age, producing only 1 steroid class. Carcinomas are usually large (> 6 cm), and only 10% are bilateral. They should be suspected mainly when the tumor presents with hypercortisolism associated with hyperandrogenism. They have a bimodal age distribution, with peaks in childhood and adolescence, as well as at the end of life [3].
Conclusion
Early identification of Cushing’s syndrome, with measures based on the assessment of risks and benefits, remains the best way to prevent progression and reduce morbidity [2]. After 6 months of drug inhibition of steroidogenesis, blood pressure control and anti-osteoporotic therapy, the objective was to minimize the levels and deleterious metabolic effects of hypercortisolism, which could also harm the surgical procedure in the short and long term through infections, dehiscence, nonimmediate bed mobilization and cardiovascular events. Unilateral adrenalectomy was chosen, given the possibility of malignancy in a young patient and to avoid definitive surgical adrenal insufficiency if the adrenalectomy was bilateral. Despite the unavailability of genetic analysis for a precise etiological definition, it is possible to take efficient measures to avoid unnecessary consequences or damage.
Pedro AO, Plapler PG, Szejnfeld VL. Manual brasileiro de osteoporose: orientações práticas para os profissionais de saúde. 1st ed. São Paulo: Editora Clannad; 2021. ISBN 978-65-89832-00-3.
Naguib R, Elkemary EZ, Elsharkawi KM. The severity of bone loss: a comparison between Cushing’s disease and Cushing’s syndrome. J Endocrinol Metab. 2023;13(1):33–8. https://doi.org/10.14740/jem857.
Wang D, Dang CX, Hao YX, Yu X, Liu PF, Li JS. Relationship between osteoporosis and Cushing syndrome based on bioinformatics. Medicine (Baltimore). 2022;101(43): e31283.
Williams TA, Reincke M. Management of Endocrine Disease: diagnosis and management of primary aldosteronism: the Endocrine Society guideline 2016 revisited. Eur J Endocrinol. 2018;179(1):R19–29. https://doi.org/10.1530/EJE-17-0990.
Compston J, Cooper A, Cooper C, Gittoes N, Gregson C, Harvey N, National Osteoporosis Guideline Group (NOGG), et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos. 2017;12(1):43. https://doi.org/10.1007/s11657-017-0324-5.
Hsiao HP, Kirschner LS, Bourdeau I, Keil MF, Boikos SA, Verma S, et al. Clinical and genetic heterogeneity, overlap with other tumor syndromes, and atypical glucocorticoid hormone secretion in adrenocorticotropin-independent macronodular adrenal hyperplasia compared with other adrenocortical tumors. J Clin Endocrinol Metab. 2009;94(8):2930–7. https://doi.org/10.1210/jc.2009-0516.
Stratakis CA, Sarlis N, Kirschner LS, Carney JA, Doppman JL, Nieman LK, et al. Paradoxical response to dexamethasone in the diagnosis of primary pigmented nodular adrenocortical disease. Ann Intern Med. 1999;131(8):585–91. https://doi.org/10.7326/0003-4819-131-8-199910190-00006.
Almeida MQ, Stratakis CA. Carney complex and other conditions associated with micronodular adrenal hyperplasias. Best Pract Res Clin Endocrinol Metab. 2010;24(6):907–14. https://doi.org/10.1016/j.beem.2010.10.006.
Serviço de Endocrinologia, Hospital Universitário da Universidade Federal de Juiz de Fora, Juiz de Fora, Minas Gerais, Brazil
Bárbara Oliveira Reis, Christianne Toledo Sousa Leal, Danielle Guedes Andrade Ezequiel, Ana Carmen dos Santos Ribeiro Simões Juliano, Flávia Lopes de Macedo Veloso, Leila Marcia da Silva, Lize Vargas Ferreira, Mariana Ferreira & Gabriel Zeferino De Oliveira Souza
Contributions
All the authors contributed to the conception and design of the work and have approved the submitted version. All authors read and approved the final manuscript.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Surgical removal of adrenal gland.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
SAN DIEGO, CA, USA I August 10, 2021 I Crinetics Pharmaceuticals, Inc. (Nasdaq: CRNX), a clinical stage pharmaceutical company focused on the discovery, development, and commercialization of novel therapeutics for rare endocrine diseases and endocrine-related tumors, today announced positive preliminary findings from the single ascending dose (SAD) portion of a first-in-human Phase 1 clinical study with CRN04894 demonstrating pharmacologic proof-of-concept for this first-in-class, investigational, oral, nonpeptide adrenocorticotropic hormone (ACTH) antagonist that is being developed for the treatment of conditions of ACTH excess, including Cushing’s disease and congenital adrenal hyperplasia.
“ACTH is the central hormone of the endocrine stress response. Even though we’ve known about its clinical significance for more than 100 years, there has never been an ACTH antagonist available to intervene in diseases of excess stress hormones. This is an important milestone for the field of endocrinology and for our company,” said Scott Struthers, Ph.D., founder and chief executive officer of Crinetics. “I am extremely proud of our team that conceived, discovered and developed CRN04894 this far. This is the second molecule to emerge from our in-house discovery efforts and demonstrate pharmacologic proof of concept. I am very excited to see what it can do in upcoming clinical studies.”
The 39 healthy volunteers who enrolled in the SAD cohorts were administered oral doses of CRN04894 (10 mg to 80 mg, or placebo) two hours prior to a challenge with synthetic ACTH. Analyses of basal cortisol levels (before ACTH challenge) showed that CRN04894 produced a rapid and dose-dependent reduction of cortisol by 25-56%. After challenge with a supra-pathophysiologic dose of ACTH (250 mcg), CRN04894 suppressed cortisol (as measured by AUC) up to 41%. After challenge with a disease-relevant dose of ACTH (1 mcg), CRN04894 showed a clinically meaningful reduction in cortisol AUC of 48%. These reductions in cortisol suggest that CRN04894 is bound with high affinity to its target receptor on the adrenal gland and blocking the activity of ACTH. CRN04894 was well tolerated in the healthy volunteers who enrolled in these SAD cohorts and all adverse events were considered mild.
“We are very encouraged by these single ascending dose data which clearly demonstrate proof of ACTH antagonism with CRN04894 exposure in healthy volunteers,” stated Alan Krasner, M.D., chief medical officer of Crinetics. “We look forward to completing this study and assessing results from the multiple ascending dose cohorts. As a clinical endocrinologist, I recognize the pioneering nature of this work and eagerly look forward to further understanding the potential of CRN04894 for the treatment of diseases of ACTH excess.”
Data Review Conference Call
Crinetics will hold a conference call and live audio webcast today, August 10, 2021 at 4:30 p.m. Eastern Time to discuss the results of the CRN04894 SAD cohorts. To participate, please dial 800-772-3714 (domestic) or 212-271-4615 (international) and refer to conference ID 21996541. To access the webcast, please visit the Events page on the Crinetics website. The archived webcast will be available for 90 days.
About the CRN04894-01 Phase 1 Study
Crinetics is enrolling healthy volunteers in this double-blind, randomized, placebo-controlled Phase 1 study of CRN04894. Participants will be divided into multiple cohorts in the single ascending dose (SAD) and multiple ascending dose (MAD) phases of the study. In the SAD phase, safety and pharmacokinetics are assessed. In addition, pharmacodynamic responses are evaluated before and after challenges with injected synthetic ACTH to assess pharmacologic effects resulting from exposure to CRN04894. In the MAD phase, participants will be administered placebo or ascending doses of study drug daily for 10 days. Assessments of safety, pharmacokinetics and pharmacodynamics will also be performed after repeat dosing.
About CRN04894
Adrenocorticotropic hormone (ACTH) is synthesized and secreted by the pituitary gland and binds to melanocortin type 2 receptor (MC2R), which is selectively expressed in the adrenal gland. This interaction of ACTH with MCR2 stimulates the adrenal production of cortisol, a stress hormone that is involved in the regulation of many systems. Cortisol is involved for example in the regulation of blood sugar levels, metabolism, inflammation, blood pressure, and memory formulation, and excess adrenal androgen production can result in hirsutism, menstrual dysfunction, infertility in men and women, acne, cardiometabolic comorbidities and insulin resistance. Diseases associated with excess of ACTH, therefore, can have significant impact on physical and mental health. Crinetics’ ACTH antagonist, CRN04894, has exhibited strong binding affinity for MC2R in preclinical models and demonstrated suppression of adrenally derived glucocorticoids and androgens that are under the control of ACTH, while maintaining mineralocorticoid production.
About Cushing’s Disease and Congenital Adrenal Hyperplasia
Cushing’s disease is a rare disease with a prevalence of approximately 10,000 patients in the United States. It is more common in women, between 30 and 50 years of age. Cushing’s disease often takes many years to diagnose and may well be under-diagnosed in the general population as many of its symptoms such as lethargy, depression, obesity, hypertension, hirsutism, and menstrual irregularity can be incorrectly attributed to other more common disorders.
Congenital adrenal hyperplasia (CAH) encompasses a set of disorders that are caused by genetic mutations that result in impaired cortisol synthesis with a prevalence of approximately 27,000 patients in the United States. This lack of cortisol leads to a loss of feedback mechanisms and results in persistently high levels of ACTH, which in turn causes overstimulation of the adrenal cortex. The resulting adrenal hyperplasia and over-secretion of other steroids (particularly androgens) and steroid precursors can lead to a variety of effects from improper gonadal development to life-threatening adrenal crisis.
About Crinetics Pharmaceuticals Crinetics Pharmaceuticals is a clinical stage pharmaceutical company focused on the discovery, development, and commercialization of novel therapeutics for rare endocrine diseases and endocrine-related tumors. The company’s lead product candidate, paltusotine, is an investigational, oral, selective nonpeptide somatostatin receptor type 2 agonist for the treatment of acromegaly, an orphan disease affecting more than 26,000 people in the United States. A Phase 3 program to evaluate safety and efficacy of paltusotine for the treatment of acromegaly is underway. Crinetics also plans to advance paltusotine into a Phase 2 trial for the treatment of carcinoid syndrome associated with neuroendocrine tumors. The company is also developing CRN04777, an investigational, oral, nonpeptide somatostatin receptor type 5 (SST5) agonist for congenital hyperinsulinism, as well as CRN04894, an investigational, oral, nonpeptide ACTH antagonist for the treatment of Cushing’s disease, congenital adrenal hyperplasia, and other diseases of excess ACTH. All of the company’s drug candidates are new chemical entities resulting from in-house drug discovery efforts and are wholly owned by the company.
Patients with adrenal insufficiency may accrue substantial health care costs and have more hospital stays and outpatient visits compared with healthy controls, according to findings published in the Journal of the Endocrine Society.
Candace Gunnarsson, PhD, vice president of health economics and outcomes research at CTI Clinical Trial and Consulting in Cincinnati, and colleagues evaluated data from a U.S.-based payer database on 10,383 patients with adrenal insufficiency to determine the estimated annual health care burden among them.
Participants were divided into groups based on their type of adrenal insufficiency: primary adrenal insufficiency (n = 1,014), adrenal insufficiency secondary to pituitary disease (n = 8,818) or congenital adrenal hyperplasia (n = 551). A group of matched controls was also evaluated for comparison.
Total annual health care expenditures were significantly higher in the primary adrenal insufficiency group ($18,624 vs. $4,320), adrenal insufficiency secondary to pituitary disease group ($32,218 vs. $6,956) and the congenital adrenal hyperplasia group ($7,677 vs. $4,203) compared with controls. The adrenal insufficiency secondary to pituitary disease group had the highest health care expenditure estimated with an incremental health care burden of $25,262, followed by the primary adrenal insufficiency group ($14,304) and the congenital adrenal hyperplasia group ($3,474).
Compared with controls, participants with adrenal insufficiency spent eight to 10 times more days in the hospital and had up to twice as many outpatient visits per year.
“When comparing [adrenal insufficiency] patients within each cohort based on their drug regimen, patients receiving prednisone therapy vs. hydrocortisone therapy had significantly higher total annual expenditures in the [primary adrenal insufficiency] and [congenital adrenal hyperplasia] and significantly lower total expenditures in the [pituitary disease] cohort,” the researchers wrote. “Patients taking only hydrocortisone and meeting the threshold of 50% adherence were found to have lower expenditures when medication adherence was 75% or higher.” – by Amber Cox
Disclosure: Gunnarsson reports being an employee of CTI Clinical Trial and Consulting. Please see the full study for a list of all other authors’ relevant financial disclosures.