


At the Annual ENDO 2017 meeting in Orlando, FL, Moore et al provided an update on somavaratan, the long acting recombinant human growth hormone being investigated for children and adults with growth hormone deficiency.
Current treatment for these patients is somewhat burdensome given the need for daily subcutaneous injections. Somavaratan provides the option for bimonthly injections.
At ENDO 2017, 3 year data was presented in children given somavaratan and the data is impressive.
The 3 year data is part of an ongoing extension study following a 6 month Phase 2 trial in which 64 patients received 5.0 mg/kg/month at various dosing schedules. Of those patients, 60 continued in an open label extension study (dose adjusted to 3.5 mg/kg given twice-monthly by the beginning of Year 2 of treatment). At ENDO 2017, data from 30 of those patients who had completed 3 years of treatment were presented.
(Insulin-like growth factor standard deviation score (IGF-I SDS) increased from -1.7 ± 0.8 at baseline to 1.1 ± 1.6 at peak (3–5 days post-injection) and -0.2 ± 0.9 at trough (end of dosing cycle) in Year 3. Of the 30 patients, 8 had transient IGF-I SDS excursions > 2.0, of which 3 events were > 3.0 (range, 2.3–3.9).

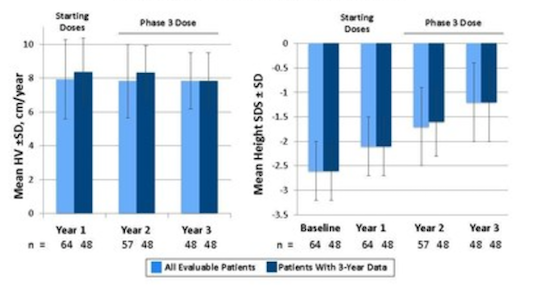
Height velocity (HV) remained consistent at 8.5 ± 1.8, 8.5 ± 1.7, and 8.1 ± 1.5 cm/year, for years 1, 2, and 3 respectively.
Height-SDS increased from -2.6 ± 0.5 at baseline to -1.9 ± 0.6, -1.4 ± 0.7, and -1.0 ± 0.7 at years 1, 2, and 3, respectively.
Treatment-related adverse events were generally mild and transient.
In an exclusive interview with Rare Disease Report, one of the investigators of the study, Bradley Miller, MD, PhD, of the University of Minnesota Masonic Children’s Hospital, said that compliance is an issue with growth hormone replacement therapy and any options that can remove the daily injection requirements would likely be well received by both patients and clinicians.
A Phase 3 study is currently underway to comparing bimonthly somavaratan treatment with daily growth hormone treatments (NCT02339090).
Somavaratan is being developed by Versartis Inc
About Growth Hormone Deficiency
Growth hormone deficiency occurs when the pituitary gland does not produce enough growth hormone, resulting in short stature, delayed or absent puberty, and changes in muscle mass, cholesterol levels, and bone strength. The condition can be congenital, structural (malformations in the brain) or acquired (resulting from trauma, infections, tumors, radiation therapy, or other causes).
Currently, the standard of care is subcutaneous injection of a biosynthetic recombinant human growth hormone (rhGH). The frequency of the injections is based on the patient’s level of growth hormone deficiency (ie, whether growth hormone is completely absent or some growth hormone is present), but most patients require daily administration.
The rhGH treatments are typically given until the child’s maximum growth potential is achieved, often requiring many years of treatment (and increasing the risk of poor compliance).
Reference
Moore WV, Fechner PY, Nguyan HJ, et al. Safety and Efficacy of Somavaratan (VRS-317), a Long-Acting Recombinant Human Growth Hormone (rhGH), in Children with Growth Hormone Deficiency (GHD): 3-Year Update of the Vertical & VISTA Trials (NCT01718041, NCT02068521). Presented at: ENDO 2017; Orlando, FL; April 1-4, 2017. Abstract OE31-1.
From http://www.raredr.com/news/bimonthly-growth-hormone
Filed under: Cushing's, pituitary | Tagged: Adult Growth Hormone Deficiency, ENDO 2017, growth hormone, IGF-1, somavaratan | Leave a comment »
