A 29-year-old Japanese pregnant woman, G5P3A1, conceived spontaneously and was referred to our hospital because of uncontrolled hypertension at 24 weeks of gestation. On admission, she presented with physical findings characteristic of Cushing’s syndrome (CS), such as moon face, buffalo hump, and reddish-purple striae. Laboratory examination revealed hyperglycemia and hypercortisolism with suppressed adrenocorticotropic hormone levels. Imaging studies revealed a right adrenocortical adenoma, and the patient was clinically diagnosed with adrenal CS. At 28 weeks, she underwent retroperitoneoscopic adrenalectomy, which normalized maternal cortisol levels and improved metabolic abnormalities. Despite these improvements, she was diagnosed with fetal growth restriction accompanied by superimposed preeclampsia at approximately 33 weeks. The maternal serum soluble fms-like kinase 1 (sFlt-1)/placental growth factor (PlGF) ratio was markedly elevated. At 36 weeks, an emergency cesarean section was performed for fetal compromise, resulting in the delivery of a small-for-gestational-age infant. Histopathological examination of the placenta revealed ischemic changes consistent with placental insufficiency. Both the mother and infant were discharged in stable conditions. The present case shows that although adrenalectomy during pregnancy can correct endocrine abnormalities, it does not necessarily prevent subsequent fetal growth restriction.
Introduction
Cushing’s syndrome (CS) is an endocrine disorder caused by chronic hypercortisolism. Because cortisol can disrupt ovulation, leading to menstrual irregularities and infertility [1,2], pregnancy in women with CS is exceedingly rare. Moreover, diagnosis during pregnancy is particularly challenging as many hallmark features of hypercortisolism – fatigue, weight gain, acne, and mood instability – are common in normal pregnancies.
Untreated CS during gestation is associated with substantially increased maternal and perinatal morbidity and mortality. Aggressive management during gestation, including cortisol synthesis inhibitors or surgical resection of pituitary adenomas or adrenal tumors, has been shown to improve maternal and fetal outcomes [3-5]. However, intensive treatment may not fully reduce the risks of fetal growth restriction and preterm delivery [5,6], and the underlying reason for this remains unclear.
Herein, we report a case of adrenal CS in a pregnant woman who underwent retroperitoneoscopic adrenalectomy at 28 weeks of gestation. Despite achieving biochemical remission of hypercortisolism after surgery, she developed fetal growth restriction and required preterm cesarean delivery due to fetal compromise.
This article was previously presented as a meeting abstract at (1) the 97th Annual Congress of the JES on June 7, 2024; (2) the 60th Annual Congress of JSPNM on July 15, 2024; and (3) the 47th Annual Meeting of JSGOS on November 24, 2024.
Case Presentation
A 29-year-old Japanese woman with a G5P3A1 conceived spontaneously. She had no medical history other than asthma and no particular familial history. She began receiving antenatal care at a nearby facility during the first trimester. She did not undergo screening tests for predicting the development of preeclampsia (PE), such as the first-trimester ultrasound at 11-14 weeks or pregnancy-associated plasma protein A assessment. Her casual blood glucose level was 87 mg/dL at 10+6 weeks of gestation. Initially, she was normotensive, but her blood pressure gradually increased to 144/100 mmHg at 18 weeks of gestation, and diagnosed as having chronic hypertension. Thereafter, her hypertension worsened, reaching 177/100 mmHg at 21 weeks of gestation, and she was diagnosed with superimposed PE. Around the same time, her body weight increased by 11.5 kg from the pre-pregnancy weight (from 58.5 kg to 70 kg), and generalized edema developed. As a result, she was admitted to the referring hospital and started taking antihypertensive treatment with oral methyldopa 750 mg/day, which lowered her blood pressure to a range of 130-150/80-100 mmHg, decreased her body weight to 66.5 kg, and improved the generalized edema. Although she was discharged from the hospital, her blood pressure increased again; thus, she was transferred to our institution, a tertiary referral perinatal medical center, at 24+6 weeks of gestation for subsequent perinatal management.
At her initial visit, her height and body weight were 153 cm and 66.2 kg, respectively. Her vital signs were as follows: body temperature 36.0℃, blood pressure 159/115 mmHg with the use of antihypertensive medication, and heart rate 80/min. She had an obvious full-moon face, acne vulgaris (Figure 1A), a buffalo hump, and reddish-purple striae on her abdomen and thighs (Figures 1B, 1C). She also had bilateral pitting edema in her lower legs and thin skin on the backs of her hands. No anemic palpebral conjunctiva, cervical lymphadenopathy, or thyroid enlargement was observed.
Figure 1: Macroscopic findings characteristic of Cushing’s syndrome
(A) Moon face, (B) reddish-purple striae
on abdomen, and (C) reddish-purple striae on thighs.
An increased neutrophil count and decreased eosinophil count were observed, although the white blood cell count was within the normal range (Table 1). Biochemical analysis showed that the serum potassium level was decreased (2.3 mEq/L). The serum total protein, albumin, blood urea nitrogen, and cholinesterase levels were mildly decreased. Renal function, hepatic function, and lipid profiles were within normal limits, except for elevated triglyceride levels. A spot urine test indicated an elevated urine protein-to-creatinine ratio (0.436 g/gCr) (Table 2). Regarding diabetes-related tests, fasting plasma glucose (91 mg/dL), glycated hemoglobin (HbA1c) (5.4%), and glycated albumin (GA) (12.9%) were all within their normal ranges. The serum C-peptide level was elevated. A 75 g oral glucose tolerance test (OGTT) conducted at 25+4 weeks of gestation showed serum glucose levels of 191 mg/dL at one hour and 212 mg/dL at two hours (Table 2), indicating postprandial hyperglycemia. Endocrinological evaluation revealed elevated morning serum cortisol levels with loss of diurnal variation. This hypercortisolism is accompanied by suppressed plasma adrenocorticotropic hormone (ACTH) levels (Table 3). The 24-hour urinary free cortisol (UFC) level was markedly elevated (1,380 μg/day). In contrast, dehydroepiandrosterone sulfate (DHEA-S) levels decreased. Serum thyroid-stimulating hormone (TSH) was markedly decreased (0.091 IU/mL), accompanied by mild reductions in free T3 (1.65 pg/mL) and free T4 (0.65 ng/dL), which indicated central hypothyroidism. Abdominal ultrasonography revealed a nodule in the right adrenal gland with a maximum diameter of approximately 30 mm (28 × 27 × 25 mm) (Figure 2A). Abdominal magnetic resonance imaging (MRI) detected a 27-mm well-defined nodular lesion at the same location, which demonstrated a signal drop on opposed-phase images (Figure 2B). Obstetric ultrasonography revealed an estimated fetal body weight of 742 g (adequate for gestational age) (Figures 3A–3C), an amniotic fluid index of 16.4 cm (Figure 3D), and no major structural anomalies of the fetus. From the day of referral, oral nifedipine (40 mg/day) was initiated as antihypertensive therapy. Potassium chloride (KCl) was administered orally.
Parameter
Test value
Reference range
CBC
WBC
8.1×109/L
3.3-8.6 ×109/L
Neut
83.5%
38.5-80.5%
Lymph
10.5%
16.5-49.5%
Mono
5.8%
2.0-10%
Eosino
0.1%
0.0-8.5%
RBC
3.17×1012/L
3.86-4.92 ×1012/L
Hb
11.5 g/dL
11.4-16.8 g/dL
Plt
190×109/L
158-348 ×109/L
Serum Biochemistry
TP
5.7 g/dL
6.6-8.1 g/dL
Alb
3.3 g/dL
4.1-5.1 g/dL
T-Bil
1 mg/dL
0.4-1.5 mg/dL
AST
15 U/L
13-30 U/L
ALT
27 U/L
7-23 U/L
LDH
326 U/L
124-222 U/L
ALP
55 U/L
38-113 U/L
γ-GTP
29 U/L
9-32 U/L
Na
146 mEq/L
138-145 mEq/L
K
2.3 mEq/L
3.6-4.8 mEq/L
Cl
107 mEq/L
101-108 mEq/L
Ca
8.5 mg/dL
8.8-10.1 mg/dL
P
2.1 mg/dL
2.7-4.6 mg/dL
BUN
6 mg/dL
8-20 mg/dL
UA
3.4 mg/dL
2.6-5.5 mg/dL
Cr
0.45 mg/dL
0.46-0.79 mg/dL
CRP
0.1 mg/dL
0-0.14 mg/dL
HDL-C
66 mg/dL
48-103 mg/dL
LDL-C
134 mg/dL
65-163 mg/dL
TG
211 mg/dL
30-117 mg/dL
FPG
91 mg/dL
73-109 mg/dL
HbA1c
5.4%
4.9-6.0%
GA
12.9%
12.3-16.5%
C-peptide
3.7 ng/mL
0.6-1.8 ng/mL
Endocrinology
Adrenaline
<0.01 ng/mL
<0.17 ng/mL
Noradrenaline
0.09 ng/mL
0.15-0.57 ng/mL
Dopamine
<0.02 ng/mL
<0.03 ng/mL
Cortisol
24.7 μg/dL
3.7-19.4 μg/dL
Aldosterone
<4.0 pg/mL
4.0-82.1 pg/mL
Renin activity
0.7 ng/mL/hr
0.2-3.9 ng/mL/hr
DHEA-S
43 μg/dL
92-399 μg/dL
TSH
0.091 IU/mL
0.350-4.940 IU/mL
FT3
1.65 pg/mL
1.68-3.67 pg/mL
FT4
0.65 ng/dL
0.70-1.48 ng/dL
Table 1: Laboratory data of CBC, serum biochemistry, and endocrinology
Table 2: Laboratory data of 75-g OGTT and urinalysis
OGTT: oral glucose tolerance test, PG: plasma glucose, IRI: immunoreactive insulin, U-Cr: urinary creatinine, U-TP: urinary total protein
Parameter
Test value
Reference range
ACTH/F diurnal rhythm
ACTH
6:00 AM
2.1 pg/mL
7.2-63.3 pg/mL
4:00 PM
2.0 pg/mL
7.2-63.3 pg/mL
11:00 PM
2.3 pg/mL
7.2-63.3 pg/mL
F
6:00 AM
24.7 μg/dL
3.7-19.4 μg/dL
4:00 PM
25 μg/dL
3.7-19.4 μg/dL
11:00 PM
25.8 μg/dL
3.7-19.4 μg/dL
Table 3: Laboratory data of ACTH/F diurnal rhythm
ACTH: adrenocorticotropic hormone, F: cortisol
Figure 2: Radiological findings of the right adrenal tumor (white arrow)
(A) Trans-abdominal ultrasonography image and (B) coronal section of the trunk on MRI.
Figure 3: Obstetric ultrasonography
(A) The plane used for biparietal diameter measurement, (B) the plane used for abdominal circumference measurement, (C) the plane used for femoral length measurement, and (D) the plane used for amniotic fluid index measurement.
Physical examination revealed typical signs of CS, such as a moon face, buffalo hump, and reddish-purple striae. In addition, laboratory findings showed elevated UFC, increased nocturnal serum cortisol levels (>5.0 μg/dL), and suppressed ACTH levels (<5.0 pg/mL). On the basis of these findings, the patient was diagnosed with ACTH-independent CS. Furthermore, imaging studies identified a right adrenal mass, leading to a final diagnosis of CS caused by a right adrenal tumor. Both central hypothyroidism and impaired glucose tolerance were considered secondary complications, primarily caused by hypercortisolemia due to CS. The serum potassium level was maintained at approximately 3.0 mEq/L after the administration of oral KCl. An increase in the nifedipine dose from 20 mg/day to 40 mg/day stabilized the blood pressure at approximately 140/90 mmHg (Figure 4A). Intensive insulin therapy with insulin lispro was initiated on hospital day 4 (Figure 4B), and the insulin dosage was gradually increased for postprandial hyperglycemia. The maximum insulin dose was 41 units/day on day 23 of hospitalization. Throughout this period, the UFC levels remained persistently elevated (Figure 4C).
Figure 4: Clinical course between hospitalization and cesarean delivery
(A) Blood pressure trend, (B) total dose of insulin, and (C) urinary free cortisol trend.
A clinical team of obstetricians, urologists, and endocrinologists discussed the treatment plans for CS and perinatal management. Pharmacological treatment had two problems: radicality and risk of fetal adrenal insufficiency due to placental passage of medication; therefore, we decided to perform adrenalectomy during pregnancy. At 28+3 weeks of gestation, a retroperitoneoscopic adrenalectomy was performed by urologists. After the induction of general anesthesia, the patient lay on the bed in a complete left lateral position (Figures 5A, 5B). Consequently, the endoscope and instrument ports were placed in the same configuration as those used in the conventional retroperitoneal approach for nonpregnant patients. Port placements were planned guided by abdominal ultrasonography to identify the uterine position, and the assistant port was positioned at a location that minimized potential interference with the uterus. The surgery was completed without complications. The operative time was 83 minutes, and bleeding was minimal. Histopathological examination indicated that the tumor was an adrenocortical adenoma (Figures 6A–6C).
Figure 5: Photograph showing the patient in the left lateral decubitus position after general anethesia
(A) Abdominal area and (B) dorsal area.
Figure 6: Histopathological findings of the right adrenal gland (A, B, C) and placenta (D)
(A) Macroscopic view of the right adrenal gland showing the normal adrenal tissue (black asterisk) and the adrenal tumor (white asterisk). (B, C) Microscopic findings of the right adrenal gland and tumor (H&E staining).
(B) Normal adrenal gland (black asterisk) and adrenal tumor (white asterisk) separated by a thin fibrous capsule (black arrow).
(C) Tumor cells with abundant eosinophilic to clear cytoplasm arranged in a trabecular to microacinar growth pattern.
(D) Microscopic findings of the placenta (H&E staining) showing fibrin deposition within villous vessels (black arrow) and chorionic villi with loss of nuclear detail and crowding (black asterisk).
After surgery, the maternal glucose tolerance rapidly improved, and intensive insulin therapy with insulin lispro became unnecessary (Figure 4B). To avoid postoperative adrenal insufficiency, replacement therapy with hydrocortisone was initiated at 200 mg/day immediately after surgery, and the dosage was gradually tapered to 25 mg/day before delivery (Figure 4C). Maternal thyroid function normalized two weeks after surgery. At 29 weeks of gestation, oral nifedipine (40 mg/day) was stopped and blood pressure was monitored; however, high blood pressure was sustained. Therefore, oral nifedipine was resumed at 20 mg/day at 31 weeks of gestation. At approximately 33 weeks of gestation, the fetus exhibited slow growth, leading to a diagnosis of fetal growth restriction. The levels of serum soluble fms-like kinase 1 (sFlt-1)/placental growth factor (PlGF) were 173 (7990/46.1) at 33+0, 299 (11600/38.9) at 34+1, and 316 (15200/48.1) at 35+5 weeks. Trends in the estimated fetal body weight and standard deviation are shown in Figure 7. At 36+1 weeks of gestation, cardiotocography revealed severely prolonged deceleration regardless of the absence of uterine contraction, and an emergency cesarean section was performed. A male infant weighing 1,726 g and 41 cm in height, diagnosed as small for gestational age, was born with Apgar scores of 8 at one minute and 9 at five minutes. The umbilical arterial pH was 7.36. The size and weight of the placenta were 14.7 × 12.8 × 3.0 cm and 315 g, respectively, and histopathological examination revealed findings consistent with ischemic infarction (Figure 6D). Antihypertensive drugs administered to the mother were discontinued on day 8. The mother and neonate were discharged on POD 20. The child achieved normal development at the age of two years.
Figure 7: Trends in estimated fetal body weight (EFBW) and standard deviation (SD)
Discussion
This case illustrates adrenal CS in pregnancy, complicated by the subsequent development of fetal growth restriction, despite retroperitoneoscopic adrenalectomy at 28 weeks of gestation. Notably, a markedly increased maternal serum sFlt-1/PlGF ratio was detected at the time of diagnosis of fetal growth restriction. To the best of our knowledge, this is the first case in which angiogenic markers were evaluated in a pregnant woman with adrenal CS.
The coexistence of CS and pregnancy is extremely rare [4]. The primary reason for this rarity is infertility, often caused by the hypercortisolism characteristic of CS. Specifically, hypercortisolism suppresses the hypothalamic-pituitary-gonadal axis, leading to impaired follicular development and anovulation by disrupting the secretion of gonadotropin-releasing hormone (GnRH) [1,7]. Pregnancy poses significant challenges in patients with ACTH-dependent CS, in whom excessive ACTH production is accompanied by androgen overproduction. As a result, adrenal etiologies of CS are more common than pituitary-dependent etiologies during pregnancy [3]. Several factors make it difficult to diagnose CS during pregnancy. First, the characteristic physical findings of CS closely mimic physiological changes in normal pregnancy. For example, weight gain, abdominal striae, and edema are common symptoms of both conditions. Therefore, this overlap can cause delayed diagnosis or misdiagnosis of CS during pregnancy [3]. It has been reported that 21.5% of pregnant women with CS are diagnosed only after delivery [3]. Second, physiological hormonal changes during pregnancy complicate the diagnostic process. During gestation, the placenta produces corticotropin-releasing hormone (CRH) and ACTH [8]. Additionally, elevated estrogen levels increase the synthesis of corticosteroid-binding globulin, resulting in a state of physiological hypercortisolism in pregnant women [9,10]. Consequently, the dexamethasone suppression test, which is key to the diagnosis of CS, is often unreliable in pregnant women because of the high incidence of false-positive results [4].
Despite these diagnostic hurdles, certain findings are highly valuable in identifying CS during pregnancy. First, careful examination of physical signs specific to CS, such as skin thinning and the presence of wide, reddish-purple striae, is crucial. Second, the evaluation of diurnal cortisol rhythms was informative. While this rhythm is preserved in normal pregnancy, it is characteristically absent in CS. Therefore, measuring late-night serum cortisol levels is useful for differentiating between these two states [11]. Third, a 24-hour UFC level exceeding three times the upper limit of normal for non-pregnant individuals is strongly suggestive of CS [4,7,9]. In the present case, these key features were decisive for the diagnosis. We found wide, reddish-purple striae, a loss of diurnal cortisol rhythm, and a markedly elevated 24-hour UFC level. Based on these findings, we definitively diagnosed the patient with CS complicating pregnancy.
According to a systematic review of 263 pregnancies complicated by CS, untreated pregnant women were significantly more likely to develop PE than those treated beforehand (26.5% vs. 2.3%) [3]. PE is characterized by defective placentation and impaired spiral artery remodeling, leading to placental ischemia during early pregnancy. Placental ischemia produces sFlt-1, a splice variant of Flt-1 that binds to vascular endothelial growth factor and PlGF and serves as a biochemical marker of endothelial dysfunction that inhibits angiogenesis [12]. Systemic endothelial dysfunction leads to maternal hypertension, proteinuria, and damage to other organs, including the placenta. In this case, placental histopathology indicated ischemic changes without retroplacental hematoma. In addition, a marked elevation of the sFlt-1/PlGF ratio – resulting from both increased sFlt-1 and decreased PlGF – was detected, supporting the presence of placental ischemia due to impaired placentation in early pregnancy.
In this case, several factors may have contributed to the placental ischemia. First, poor control of maternal hyperglycemia or hypertension may have played a role. As hyperglycemia is known to induce oxidative stress [13], it is possible that hyperglycemia in early pregnancy causes placental ischemia indirectly via oxidative stress. Recent studies suggest that hypertension in early pregnancy may contribute to impaired placentation, thereby increasing the risk of subsequent superimposed PE [14,15]. Therefore, chronic hypertension associated with CS may also be related to placental ischemia, although the maternal outpatient blood pressure was within the normal range during early pregnancy in the present case. Second, chronic hypercortisolemia can directly contribute to abnormal placentation. Previous animal experiments have shown that elevated maternal serum cortisol levels enhance uterine arterial contractions [16], which may induce placental ischemia. Furthermore, chronic hypercortisolism may exceed the protective capacity of 11β-hydroxysteroid dehydrogenase type 2 (11β-HSD2), which shields the fetus from excessive cortisol, thereby directly affecting the fetus [17]. Based on these findings, it is presumed that irreversible placental damage had already occurred at the time of the surgical resection in this case. Preconceptional or at least early diagnosis and treatment of CS are crucial for preventing fetal growth restriction associated with superimposed PE after surgery.
The second trimester is generally considered the optimal period for adrenalectomy in pregnant patients with adrenal CS [18]; however, successful procedures have been reported even during the third trimester [6,19]. Endoscopic adrenalectomy is favored over open approaches owing to its reduced morbidity, although direct comparisons between the transperitoneal and retroperitoneal approaches in pregnancy are lacking. In non-pregnant patients, both approaches yield similar operative times, blood loss, and hospital stays [20]. In this case, the retroperitoneal approach was used. This technique offers several advantages during pregnancy as follows: it allows surgery in the lateral position, minimizes inferior vena cava compression by the gravid uterus, avoids entry into the peritoneal cavity, thereby preventing interference from the enlarged uterus, and reduces the risk of intra-abdominal inflammatory spread to the uterus and adjacent organs. Based on our experience and considering the potential advantages of the retroperitoneoscopic approach, we propose that retroperitoneoscopic adrenalectomy should be considered even in the early third trimester, as it may safely prolong gestation and reduce the need for preterm delivery.
Conclusions
This case highlights the challenges of managing adrenal CS during pregnancy. Uncontrolled CS may impair placental development during early pregnancy; therefore, preconceptional or at least early recognition and appropriate management are crucial to minimize the risk of subsequent fetal growth restriction. Further research is needed to clarify the pathophysiological relationship between hypercortisolism and impaired placentation in early pregnancy and to refine strategies for managing this rare but high-risk condition.
Cushing’s syndrome (CS) arises from an excess of endogenous or exogenous cortisol, with Cushing’s disease specifically implicating a pituitary adenoma and exaggerated adrenocorticotropic hormone (ACTH) production. Typically, Cushing’s disease presents with characteristic symptoms such as weight gain, central obesity, moon face, and buffalo hump.
This case report presents an unusual manifestation of CS in a 48-year-old male with a history of hypertension, where severe hypokalemia was the primary presentation. Initial complaints included bilateral leg swelling, muscle weakness, occasional shortness of breath, and a general feeling of not feeling well. Subsequent investigations revealed hypokalemia, metabolic alkalosis, and an abnormal response to dexamethasone suppression, raising concerns about hypercortisolism. Further tests, including 24-hour urinary free cortisol and ACTH testing, confirmed significant elevations. Brain magnetic resonance imaging (MRI) identified a pituitary macroadenoma, necessitating neurosurgical intervention.
This case underscores the rarity of CS presenting with severe hypokalemia, highlighting the diagnostic challenges and the crucial role of a collaborative approach in managing such intricate cases.
Introduction
Cushing’s syndrome (CS), characterized by excessive cortisol production, is well-known for its diverse and often conspicuous clinical manifestations. Cushing’s disease is a subset of CS resulting from a pituitary adenoma overproducing adrenocorticotropic hormone (ACTH), leading to heightened cortisol secretion. The classic presentation involves a spectrum of symptoms such as weight gain, central obesity, muscle weakness, and mood alterations [1].
Despite its classic presentation, CS can demonstrate diverse and atypical features, challenging conventional diagnostic paradigms. This case report sheds light on a rare manifestation of CS, where severe hypokalemia was the primary clinical indicator. Notably, instances of CS prominently manifesting through severe hypokalemia are scarce in the literature [1,2].
Through this exploration, we aim to provide valuable insights into the diagnostic intricacies of atypical CS presentations, underscore the significance of a comprehensive workup, and emphasize the collaborative approach essential for managing such uncommon hormonal disorders.
Case Presentation
A 48-year-old male with a history of hypertension presented to his primary care physician with complaints of bilateral leg swelling, occasional shortness of breath, dizziness, and a general feeling of malaise persisting for 10 days. The patient reported increased water intake and urinary frequency without dysuria. The patient was diagnosed with hypertension eight months ago. He experienced progressive muscle weakness over two months, hindering his ability to perform daily activities, including using the bathroom. The primary care physician initiated a blood workup that revealed severe hypokalemia with a potassium level of 1.3 mmol/L (reference range: 3.6 to 5.2 mmol/L), prompting referral to the hospital.
Upon admission, the patient was hypertensive with a blood pressure of 180/103 mmHg, a heart rate of 71 beats/minute, a respiratory rate of 18 breaths/minute, and an oxygen saturation of 96% on room air. Physical examination revealed fine tremors, bilateral 2+ pitting edema in the lower extremities up to mid-shin, abdominal distension with normal bowel sounds, and bilateral reduced air entry in the bases of the lungs on auscultation. The blood work showed the following findings (Table 1).
Parameter
Result
Reference Range
Potassium (K)
1.8 mmol/L
3.5-5.0 mmol/L
Sodium (Na)
144 mmol/L
135-145 mmol/L
Magnesium (Mg)
1.3 mg/dL
1.7-2.2 mg/dL
Hemoglobin (Hb)
15.5 g/dL
13.8-17.2 g/dL
White blood cell count (WBC)
13,000 x 103/µL
4.5 to 11.0 × 109/L
Platelets
131,000 x 109/L
150-450 x 109/L
pH
7.57
7.35-7.45
Bicarbonate (HCO3)
46 mmol/L
22-26 mmol/L
Lactic acid
4.2 mmol/L
0.5-2.0 mmol/L
Table 1: Blood work findings
In order to correct the electrolyte imbalances, the patient received intravenous (IV) magnesium and potassium replacement and was later transitioned to oral. The patient was also started on normal saline at 100 cc per hour. To further investigate the complaint of shortness of breath, the patient underwent a chest X-ray, which revealed bilateral multilobar pneumonia (Figure 1). He was subsequently treated with ceftriaxone (1 g IV daily) and clarithromycin (500 mg twice daily) for seven days.
Figure 1: A chest X-ray revealing (arrows) bilateral multilobar pneumonia
With persistent abdominal pain and lactic acidosis, a computed tomography (CT) scan abdomen and pelvis with contrast was conducted, revealing a psoas muscle hematoma. Subsequent magnetic resonance imaging (MRI) depicted an 8×8 cm hematoma involving the left psoas and iliacus muscles. The interventional radiologist performed drainage of the hematoma involving the left psoas and iliacus muscles (Figure 2).
Figure 2: Magnetic resonance imaging (MRI) depicting an 8×8 cm hematoma (arrow) involving the left psoas and iliacus muscles
In light of the concurrent presence of hypokalemia, hypertension, and metabolic alkalosis, there arose concerns about Conn’s syndrome, prompting consultation with endocrinology. Their recommended workup for Conn’s syndrome included assessments of the aldosterone-renin ratio and random cortisol levels. The results unveiled an aldosterone level below 60 pmol/L (reference range: 190 to 830 pmol/L in SI units) and a plasma renin level of 0.2 pmol/L (reference range: 0.7 to 3.3 mcg/L/hr in SI units). Notably, the aldosterone-renin ratio was low, conclusively ruling out Conn’s syndrome. The random cortisol level was notably elevated at 1334 nmol/L (reference range: 140 to 690 nmol/L).
Furthermore, a low-dose dexamethasone suppression test was undertaken due to the high cortisol levels. Following the administration of 1 mg of dexamethasone at 10 p.m., cortisol levels were measured at 9 p.m., 3 a.m., and 9 a.m. the following day. The results unveiled a persistently elevated cortisol level surpassing 1655 nmol/L, signaling an abnormal response to dexamethasone suppression and raising concerns about a hypercortisolism disorder, such as CS.
In the intricate progression of this case, the investigation delved deeper with a 24-hour urinary free cortisol level, revealing a significant elevation at 521 mcg/day (reference range: 10 to 55 mcg/day). Subsequent testing of ACTH portrayed a markedly elevated level of 445 ng/L, distinctly exceeding the normal reference range of 7.2 to 63.3 ng/L. A high-dose 8 mg dexamethasone test was performed to ascertain the source of excess ACTH production. The baseline serum cortisol levels before the high-dose dexamethasone suppression test were 1404 nmol/L, which decreased to 612 nmol/L afterward, strongly suggesting the source of excess ACTH production to be in the pituitary gland.
A CT scan of the adrenal glands ruled out adrenal mass, while an MRI of the brain uncovered a 1.3×1.3×3.2 cm pituitary macroadenoma (Figure 3), leading to compression of adjacent structures. Neurosurgery was consulted, and they recommended surgical removal of the macroadenoma due to the tumor size and potential complications. The patient was referred to a tertiary care hospital for pituitary adenoma removal.
Figure 3: Magnetic resonance imaging (MRI) of the brain depicting a 1.3×1.3×3.2 cm pituitary macroadenoma (star)
Discussion
CS represents a complex endocrine disorder characterized by excessive cortisol production. While the classic presentation of CS includes weight gain, central obesity, and muscle weakness, our case highlights an uncommon initial manifestation: severe hypokalemia. This atypical presentation underscores the diverse clinical spectrum of CS and the challenges it poses in diagnosis and management [1,2].
While CS typically presents with the classic symptoms mentioned above, severe hypokalemia as the initial manifestation is exceedingly rare. Hypokalemia in CS often results from excess cortisol-mediated activation of mineralocorticoid receptors, leading to increased urinary potassium excretion and renal potassium wasting. Additionally, metabolic alkalosis secondary to cortisol excess further exacerbates hypokalemia [3,4].
Diagnosing a case of Cushing’s disease typically commences with a thorough examination of the patient’s medical history and a comprehensive physical assessment aimed at identifying characteristic manifestations such as central obesity, facial rounding, proximal muscle weakness, and increased susceptibility to bruising. Essential to confirming the diagnosis are laboratory examinations, which involve measuring cortisol levels through various tests, including 24-hour urinary free cortisol testing, late-night salivary cortisol testing, and dexamethasone suppression tests. Furthermore, assessing plasma ACTH levels aids in distinguishing between pituitary-dependent and non-pituitary causes of CS. Integral to the diagnostic process are imaging modalities such as MRI of the pituitary gland, which facilitate the visualization of adenomas and the determination of their size and precise location [1-4].
Treatment for Cushing’s disease primarily entails surgical removal of the pituitary adenoma via transsphenoidal surgery, with the aim of excising the tumor and restoring normal pituitary function. In cases where surgical intervention is unsuitable or unsuccessful, pharmacological therapies employing medications such as cabergoline (a dopamine receptor agonist) or pasireotide (a somatostatin analogue) may be considered to suppress ACTH secretion and regulate cortisol levels. Additionally, radiation therapy, whether conventional or stereotactic radiosurgery, serves as a supplementary or alternative treatment approach to reduce tumor dimensions and mitigate ACTH production [5,6]. To assess the effectiveness of treatment, manage any problem, and assure long-term illness remission, diligent long-term follow-up and monitoring are essential. Collaborative multidisciplinary care involving specialists such as endocrinologists, neurosurgeons, and other healthcare professionals is pivotal in optimizing patient outcomes and enhancing overall quality of life [2,4].
The prognosis of CS largely depends on the underlying cause, stage of the disease, and efficacy of treatment. Early recognition and prompt intervention are essential for improving outcomes and minimizing long-term complications. Surgical resection of the adrenal or pituitary tumor can lead to remission of CS in the majority of cases. However, recurrence rates vary depending on factors such as tumor size, invasiveness, and completeness of resection [2,3]. Long-term follow-up with endocrinologists is crucial for monitoring disease recurrence, assessing hormonal function, and managing comorbidities associated with CS.
Conclusions
In conclusion, our case report highlights the rarity of severe hypokalemia as the initial presentation of CS. This unique presentation underscores the diverse clinical manifestations of CS and emphasizes the diagnostic challenges encountered in clinical practice. A multidisciplinary approach involving endocrinologists, neurosurgeons, and radiologists is essential for the timely diagnosis and management of CS. Early recognition, prompt intervention, and long-term follow-up are essential for optimizing outcomes and improving the quality of life for patients with this endocrine disorder.
Cushing’s syndrome (CS) arises from an excess of endogenous or exogenous cortisol, with Cushing’s disease specifically implicating a pituitary adenoma and exaggerated adrenocorticotropic hormone (ACTH) production. Typically, Cushing’s disease presents with characteristic symptoms such as weight gain, central obesity, moon face, and buffalo hump.
This case report presents an unusual manifestation of CS in a 48-year-old male with a history of hypertension, where severe hypokalemia was the primary presentation. Initial complaints included bilateral leg swelling, muscle weakness, occasional shortness of breath, and a general feeling of not feeling well. Subsequent investigations revealed hypokalemia, metabolic alkalosis, and an abnormal response to dexamethasone suppression, raising concerns about hypercortisolism. Further tests, including 24-hour urinary free cortisol and ACTH testing, confirmed significant elevations. Brain magnetic resonance imaging (MRI) identified a pituitary macroadenoma, necessitating neurosurgical intervention.
This case underscores the rarity of CS presenting with severe hypokalemia, highlighting the diagnostic challenges and the crucial role of a collaborative approach in managing such intricate cases.
Introduction
Cushing’s syndrome (CS), characterized by excessive cortisol production, is well-known for its diverse and often conspicuous clinical manifestations. Cushing’s disease is a subset of CS resulting from a pituitary adenoma overproducing adrenocorticotropic hormone (ACTH), leading to heightened cortisol secretion. The classic presentation involves a spectrum of symptoms such as weight gain, central obesity, muscle weakness, and mood alterations [1].
Despite its classic presentation, CS can demonstrate diverse and atypical features, challenging conventional diagnostic paradigms. This case report sheds light on a rare manifestation of CS, where severe hypokalemia was the primary clinical indicator. Notably, instances of CS prominently manifesting through severe hypokalemia are scarce in the literature [1,2].
Through this exploration, we aim to provide valuable insights into the diagnostic intricacies of atypical CS presentations, underscore the significance of a comprehensive workup, and emphasize the collaborative approach essential for managing such uncommon hormonal disorders.
Case Presentation
A 48-year-old male with a history of hypertension presented to his primary care physician with complaints of bilateral leg swelling, occasional shortness of breath, dizziness, and a general feeling of malaise persisting for 10 days. The patient reported increased water intake and urinary frequency without dysuria. The patient was diagnosed with hypertension eight months ago. He experienced progressive muscle weakness over two months, hindering his ability to perform daily activities, including using the bathroom. The primary care physician initiated a blood workup that revealed severe hypokalemia with a potassium level of 1.3 mmol/L (reference range: 3.6 to 5.2 mmol/L), prompting referral to the hospital.
Upon admission, the patient was hypertensive with a blood pressure of 180/103 mmHg, a heart rate of 71 beats/minute, a respiratory rate of 18 breaths/minute, and an oxygen saturation of 96% on room air. Physical examination revealed fine tremors, bilateral 2+ pitting edema in the lower extremities up to mid-shin, abdominal distension with normal bowel sounds, and bilateral reduced air entry in the bases of the lungs on auscultation. The blood work showed the following findings (Table 1).
Parameter
Result
Reference Range
Potassium (K)
1.8 mmol/L
3.5-5.0 mmol/L
Sodium (Na)
144 mmol/L
135-145 mmol/L
Magnesium (Mg)
1.3 mg/dL
1.7-2.2 mg/dL
Hemoglobin (Hb)
15.5 g/dL
13.8-17.2 g/dL
White blood cell count (WBC)
13,000 x 103/µL
4.5 to 11.0 × 109/L
Platelets
131,000 x 109/L
150-450 x 109/L
pH
7.57
7.35-7.45
Bicarbonate (HCO3)
46 mmol/L
22-26 mmol/L
Lactic acid
4.2 mmol/L
0.5-2.0 mmol/L
Table 1: Blood work findings
In order to correct the electrolyte imbalances, the patient received intravenous (IV) magnesium and potassium replacement and was later transitioned to oral. The patient was also started on normal saline at 100 cc per hour. To further investigate the complaint of shortness of breath, the patient underwent a chest X-ray, which revealed bilateral multilobar pneumonia (Figure 1). He was subsequently treated with ceftriaxone (1 g IV daily) and clarithromycin (500 mg twice daily) for seven days.
Figure 1: A chest X-ray revealing (arrows) bilateral multilobar pneumonia
With persistent abdominal pain and lactic acidosis, a computed tomography (CT) scan abdomen and pelvis with contrast was conducted, revealing a psoas muscle hematoma. Subsequent magnetic resonance imaging (MRI) depicted an 8×8 cm hematoma involving the left psoas and iliacus muscles. The interventional radiologist performed drainage of the hematoma involving the left psoas and iliacus muscles (Figure 2).
Figure 2: Magnetic resonance imaging (MRI) depicting an 8×8 cm hematoma (arrow) involving the left psoas and iliacus muscles
In light of the concurrent presence of hypokalemia, hypertension, and metabolic alkalosis, there arose concerns about Conn’s syndrome, prompting consultation with endocrinology. Their recommended workup for Conn’s syndrome included assessments of the aldosterone-renin ratio and random cortisol levels. The results unveiled an aldosterone level below 60 pmol/L (reference range: 190 to 830 pmol/L in SI units) and a plasma renin level of 0.2 pmol/L (reference range: 0.7 to 3.3 mcg/L/hr in SI units). Notably, the aldosterone-renin ratio was low, conclusively ruling out Conn’s syndrome. The random cortisol level was notably elevated at 1334 nmol/L (reference range: 140 to 690 nmol/L).
Furthermore, a low-dose dexamethasone suppression test was undertaken due to the high cortisol levels. Following the administration of 1 mg of dexamethasone at 10 p.m., cortisol levels were measured at 9 p.m., 3 a.m., and 9 a.m. the following day. The results unveiled a persistently elevated cortisol level surpassing 1655 nmol/L, signaling an abnormal response to dexamethasone suppression and raising concerns about a hypercortisolism disorder, such as CS.
In the intricate progression of this case, the investigation delved deeper with a 24-hour urinary free cortisol level, revealing a significant elevation at 521 mcg/day (reference range: 10 to 55 mcg/day). Subsequent testing of ACTH portrayed a markedly elevated level of 445 ng/L, distinctly exceeding the normal reference range of 7.2 to 63.3 ng/L. A high-dose 8 mg dexamethasone test was performed to ascertain the source of excess ACTH production. The baseline serum cortisol levels before the high-dose dexamethasone suppression test were 1404 nmol/L, which decreased to 612 nmol/L afterward, strongly suggesting the source of excess ACTH production to be in the pituitary gland.
A CT scan of the adrenal glands ruled out adrenal mass, while an MRI of the brain uncovered a 1.3×1.3×3.2 cm pituitary macroadenoma (Figure 3), leading to compression of adjacent structures. Neurosurgery was consulted, and they recommended surgical removal of the macroadenoma due to the tumor size and potential complications. The patient was referred to a tertiary care hospital for pituitary adenoma removal.
Figure 3: Magnetic resonance imaging (MRI) of the brain depicting a 1.3×1.3×3.2 cm pituitary macroadenoma (star)
Discussion
CS represents a complex endocrine disorder characterized by excessive cortisol production. While the classic presentation of CS includes weight gain, central obesity, and muscle weakness, our case highlights an uncommon initial manifestation: severe hypokalemia. This atypical presentation underscores the diverse clinical spectrum of CS and the challenges it poses in diagnosis and management [1,2].
While CS typically presents with the classic symptoms mentioned above, severe hypokalemia as the initial manifestation is exceedingly rare. Hypokalemia in CS often results from excess cortisol-mediated activation of mineralocorticoid receptors, leading to increased urinary potassium excretion and renal potassium wasting. Additionally, metabolic alkalosis secondary to cortisol excess further exacerbates hypokalemia [3,4].
Diagnosing a case of Cushing’s disease typically commences with a thorough examination of the patient’s medical history and a comprehensive physical assessment aimed at identifying characteristic manifestations such as central obesity, facial rounding, proximal muscle weakness, and increased susceptibility to bruising. Essential to confirming the diagnosis are laboratory examinations, which involve measuring cortisol levels through various tests, including 24-hour urinary free cortisol testing, late-night salivary cortisol testing, and dexamethasone suppression tests. Furthermore, assessing plasma ACTH levels aids in distinguishing between pituitary-dependent and non-pituitary causes of CS. Integral to the diagnostic process are imaging modalities such as MRI of the pituitary gland, which facilitate the visualization of adenomas and the determination of their size and precise location [1-4].
Treatment for Cushing’s disease primarily entails surgical removal of the pituitary adenoma via transsphenoidal surgery, with the aim of excising the tumor and restoring normal pituitary function. In cases where surgical intervention is unsuitable or unsuccessful, pharmacological therapies employing medications such as cabergoline (a dopamine receptor agonist) or pasireotide (a somatostatin analogue) may be considered to suppress ACTH secretion and regulate cortisol levels. Additionally, radiation therapy, whether conventional or stereotactic radiosurgery, serves as a supplementary or alternative treatment approach to reduce tumor dimensions and mitigate ACTH production [5,6]. To assess the effectiveness of treatment, manage any problem, and assure long-term illness remission, diligent long-term follow-up and monitoring are essential. Collaborative multidisciplinary care involving specialists such as endocrinologists, neurosurgeons, and other healthcare professionals is pivotal in optimizing patient outcomes and enhancing overall quality of life [2,4].
The prognosis of CS largely depends on the underlying cause, stage of the disease, and efficacy of treatment. Early recognition and prompt intervention are essential for improving outcomes and minimizing long-term complications. Surgical resection of the adrenal or pituitary tumor can lead to remission of CS in the majority of cases. However, recurrence rates vary depending on factors such as tumor size, invasiveness, and completeness of resection [2,3]. Long-term follow-up with endocrinologists is crucial for monitoring disease recurrence, assessing hormonal function, and managing comorbidities associated with CS.
Conclusions
In conclusion, our case report highlights the rarity of severe hypokalemia as the initial presentation of CS. This unique presentation underscores the diverse clinical manifestations of CS and emphasizes the diagnostic challenges encountered in clinical practice. A multidisciplinary approach involving endocrinologists, neurosurgeons, and radiologists is essential for the timely diagnosis and management of CS. Early recognition, prompt intervention, and long-term follow-up are essential for optimizing outcomes and improving the quality of life for patients with this endocrine disorder.
The diagnosis of Cushing’s syndrome is challenging; however, through the clinical picture and the search for secondary causes of osteoporosis, it was possible to reach the diagnosis of the case reported. There was an independent, symptomatic ACTH hypercortisolism manifested by typical phenotypic changes, severe secondary osteoporosis and arterial hypertension in a young patient.
Case presentation
A 20-year-old Brazilian man with low back pain for 8 months. Radiographs showed fragility fractures in the thoracolumbar spine, and bone densitometry showed osteoporosis, especially when evaluating the Z Score (− 5.6 in the lumbar spine). On physical examination, there were wide violaceous streaks on the upper limbs and abdomen, plethora and fat increase in the temporal facial region, hump, ecchymosis on limbs, hypotrophy of arms and thighs, central obesity and kyphoscoliosis. His blood pressure was 150 × 90 mmHg. Cortisol after 1 mg of dexamethasone (24.1 µg/dL) and after Liddle 1 (28 µg/dL) were not suppressed, despite normal cortisoluria. Tomography showed bilateral adrenal nodules with more severe characteristics. Unfortunately, through the catheterization of adrenal veins, it was not possible to differentiate the nodules due to the achievement of cortisol levels that exceeded the upper limit of the dilution method. Among the hypotheses for the differential diagnosis of bilateral adrenal hyperplasia are primary bilateral macronodular adrenal hyperplasia, McCune–Albright syndrome and isolated bilateral primary pigmented nodular hyperplasia or associated with Carney’s complex. In this case, primary pigmented nodular hyperplasia or carcinoma became important etiological hypotheses when comparing the epidemiology in a young man and the clinical-laboratory-imaging findings of the differential diagnoses. After 6 months of drug inhibition of steroidogenesis, blood pressure control and anti-osteoporotic therapy, the levels and deleterious metabolic effects of hypercortisolism, which could also impair adrenalectomy in the short and long term, were reduced. Left adrenalectomy was chosen, given the possibility of malignancy in a young patient and to avoid unnecessary definitive surgical adrenal insufficiency if the adrenalectomy was bilateral. Anatomopathology of the left gland revealed expansion of the zona fasciculate with multiple nonencapsulated nodules.
Conclusion
The early identification of Cushing’s syndrome, with measures based on the assessment of risks and benefits, remains the best way to prevent its progression and reduce the morbidity of the condition. Despite the unavailability of genetic analysis for a precise etiological definition, it is possible to take efficient measures to avoid future damage.
Cushing’s syndrome may be exogenous or endogenous and, in this case, can be ACTH-dependent or independent. In the case reported, there was an independent, symptomatic ACTH hypercortisolism manifested by typical phenotypic changes, severe secondary osteoporosis and arterial hypertension in a young patient. Osteoporosis secondary to hypercortisolism occurs due to chronic reduction in bone formation, loss of osteocytes and increased reabsorption caused by intense binding of cortisol to glucocorticoid receptors present in bone cells [1]. In addition, excess cortisol impairs vitamin D metabolism and reduces endogenous parathyroid hormone secretion, intestinal calcium reabsorption, growth hormone release, and lean body mass [2]. Subclinical Cushing disease occurs in up to 11% of individuals diagnosed with early-onset osteoporosis and 0.5–1% of hypertension patients. [3] A cross-sectional study published in 2023 revealed a prevalence of 81.5% bone loss in 19 patients with Cushing’s syndrome [2]. The prevalence of osteopenia ranges from 60 to 80%, and the prevalence of osteoporosis ranges from 30 to 65% in patients with Cushing’s syndrome. Additionally, the incidence of fragility fractures ranges from 30 to 50% in these patients [4] and is considered the main cause of morbidity affecting the quality of life. The diagnosis is challenging, given the presence of confounding factors; however, through the clinical picture and the search for secondary causes of osteoporosis, it was possible to reach a syndromic diagnosis. Early identification of this syndrome, with measures based on the assessment of risks and benefits, remains the best way to prevent progression and reduce morbidity related to this disease [2].
Case presentation
A 20-year-old Brazilian male patient reported low back pain that had evolved for 8 months, with no related trauma. He sought emergency care and performed spinal radiographs on this occasion (03/2019). Due to the several alterations observed in the images, he was referred to the Orthopedics Service of the Hospital of Federal University of Juiz de Fora, which prescribed orthopedic braces, indicated physical therapy and was referred again to the Osteometabolic Diseases outpatient clinic of the Endocrinology and Rheumatology Services of the Hospital of Federal University of Juiz de Fora on 10/2019.
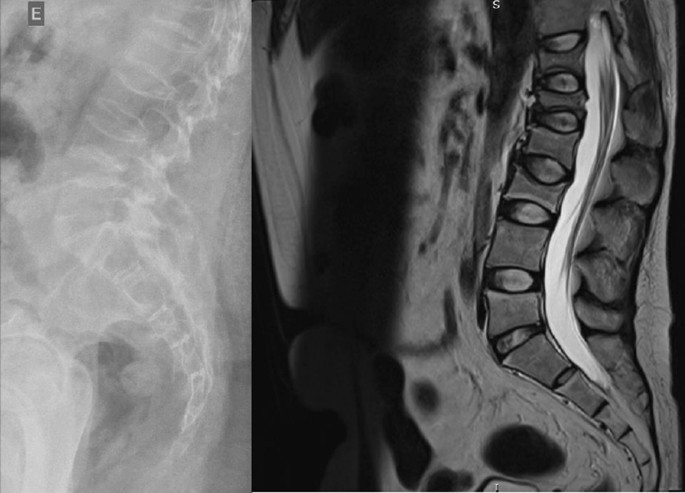
The radiographs showed a marked reduction in the density of bone structures, scoliotic deviation with convexity toward the left and reduction in the height of the lumbar vertebrae, with partial collapses of the vertebral bodies at the level of T12, L1, L2, L3 and L5, with recent collapses in T12 and L1, suggesting bone fragility fractures. The same can be seen in posterior magnetic resonance imaging (Fig. 1).
Fig. 1
Radiography and Magnetic Resonance Imaging (MRI) of lumbosacral spine in profile
Bone scintigraphy on 08/2019 did not reveal hyper flow or anomalous hyperemia in the topography of the thoracolumbar spine, and in the later images of the exam, there was a greater relative uptake of the tracer in the lumbar spine (vertebrae T10–T12, L2–L4), of nonspecific aspect, questioning the presence of osteoarticular processes or ankylosing spondylitis.
It was also observed in the bone densitometry requested in October 2019, performed by dual-energy X-ray absorptiometry (DXA), low bone mineral density (BMD) in the lumbar spine, femoral neck and total femur, when comparing the results to evaluating the Z Score (Table 1).
Thus, the diagnosis of osteoporosis was established, and treatment with vitamin D 7000 IU per week was started due to vitamin D3 insufficiency associated with the bisphosphonate alendronate 70 mg, also weekly. The patient had a past pathological history of fully treated syphilis (2018) and perianal condyloma with a surgical resection on 09/2017 and 02/2018. In the family history, it was reported that a maternal uncle died of systemic sclerosis. In the social context, the young person denied drinking alcohol and previous or current smoking.
On physical examination, there were no lentiginous skin areas or blue nevi; however, wide violet streaks were observed on the upper limbs and abdomen, with plethora and increased fat in the temporal facial region and hump (Fig. 2a, b), limb ecchymosis, hypotrophy of the arms and thighs, central obesity and kyphoscoliosis. Systemic blood pressure (sitting) was 150 × 90 mmHg, BMI was 26.09 kg/m2, and waist circumference was 99 cm, with no reported reduction in height, maintained at 1.55 m.
Fig. 2
Changes in the physical examination. a Violet streaks on the upper limbs, b Violet streaks on abdomen
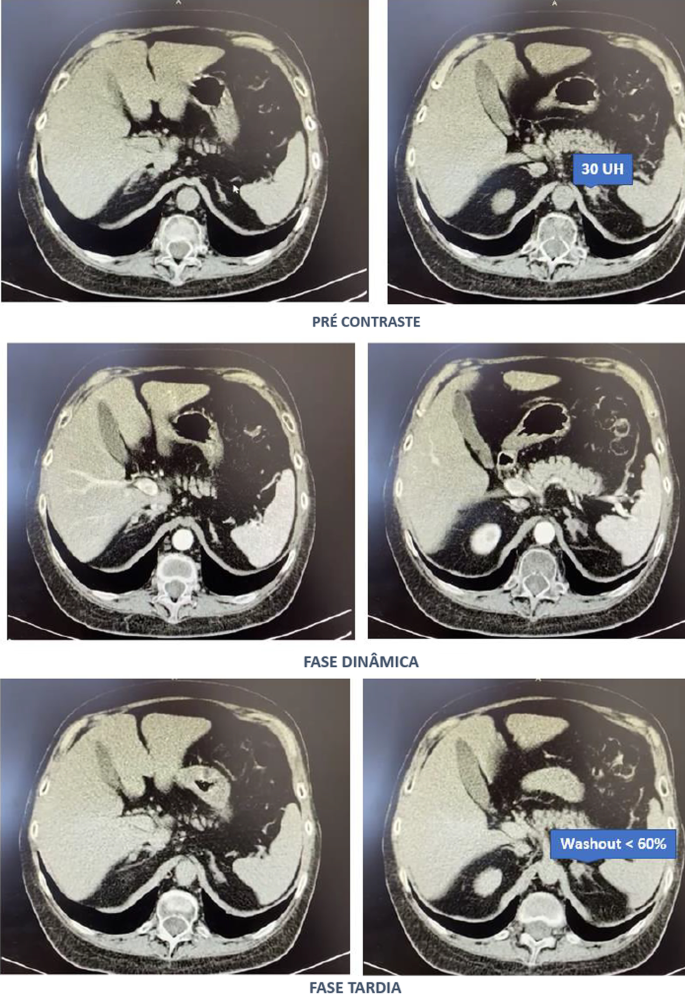
Computed tomography of the abdomen with adrenal protocol performed on 08/13/2020 characterized isodense nodular formation in the body of the left adrenal and in the lateral portion of the right adrenal, measuring 1.5 cm and 0.6 cm, respectively. The lesions had attenuation of approximately 30 HU, showing enhancement by intravenous contrast, with an indeterminate washout pattern in the late phase after contrast (< 60%) (Fig. 3).
After contact with the interventional radiology of the Hospital of Federal University of Juiz de Fora, catheterization of adrenal veins was performed on 10/2020; however, it was not possible to perform adequate lesion characterization due to obtaining serum cortisol levels that extrapolated the dilutional upper limit of the method (Table 3).
The calculation of the selectivity index was 6.63 (Reference Value (RV) > 3), confirming the good positioning of the catheter within the vessels during the procedure. The calculated lateralization index was 1.1296 (VR < 3), denoting bilateral hormone production. However, as aldosterone was not collected from a peripheral vein, it was not possible to obtain the contralateral rate and define whether there was contralateral suppression of aldosterone production [5].
Due to pending diagnoses for a better therapeutic decision and Cushing’s syndrome in clear evolution and causing organic damage, it was decided, after catheterization, to make changes in the patient’s drug prescription. Ketoconazole 400 mg per day was started, the dose of vitamin D was increased to 14,000 IU per week, and ramipril 5 mg per day was prescribed due to secondary hypertension. In addition, given the severity of osteoporosis, it was decided to replace previously prescribed alendronate with zoledronic acid.
Magnetic resonance imaging of the upper abdomen was performed on 06/19/2021, which demonstrated lobulated nodular thickening in the left adrenal gland with areas of decreased signal intensity in the T1 out-phase sequence, denoting the presence of fat, and homogeneous enhancement using contrast, measuring approximately 1.7 × 1.5 × 1.3 cm, suggestive of an adenoma. There was also a small nodular thickening in the lateral arm of the right adrenal, measuring approximately 0.8 × 0.6 cm, which was difficult to characterize due to its small dimensions and nonspecific appearance.
PPNAD or carcinoma became an important etiological hypothesis for the case described when comparing the epidemiology in a young man and the clinical-laboratory-imaging findings of the differential diagnoses. According to a dialog with the patient and family, the group of experts opted for unilateral glandular surgical resection on the left side (11/11/2021), where more significant changes were visualized, as there was a possibility of malignancy in a young patient and to avoid a definitive adrenal insufficiency condition because of bilateral adrenalectomy. This would first allow the analysis of the material and follow-up of the evolution of the condition with the permanence of the contralateral gland.
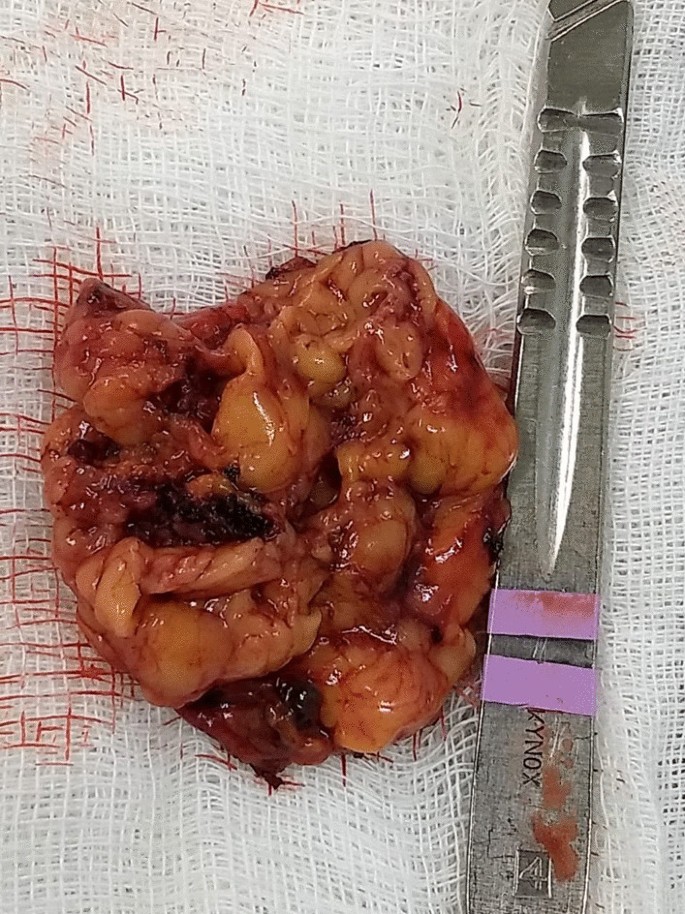
In the macroscopic analysis of the adrenalectomy specimen, adrenal tissue weighing 20 g and measuring 9.3 × 5.5 × 2.0 cm was described, completely surrounded by adipose tissue. The gland has a multinodular surface and varies between 0.2 and 1.6 cm in thickness, showing a cortex of 0.1 cm in thickness and a medulla of 1.5 cm in thickness (Fig. 4).
The microscopic analysis described the expansion of the zona fasciculate, with the formation of multiple nonencapsulated nodules composed of polygonal cells with ample and eosinophilic cytoplasm and frequent depletion of intracytoplasmic lipid content. No areas of necrosis or mitotic activity were observed. The histopathological picture is suggestive of cortical pigmented micronodular hyperplasia of the adrenal gland.
For the final etiological definition and an indication of contralateral adrenalectomy, which could be unnecessary and would avoid chronic corticosteroid therapy, or else, it would be necessary to protect the patient from future complications with the maintenance of the disease in the right adrenal gland, it would be essential to search for mutations in the PRKAR1A, PDE11A, PDE8B and PRKACA genes [15]; however, such genetic analysis is not yet widely available, and the impossibility of carrying it out at the local level did not allow a complete conclusion of the case.
Discussion
Through the clinical picture presented and the research of several secondary causes for osteoporosis, it was possible to arrive at the diagnosis of Cushing syndrome [6]. There was symptomatic independent ACTH hypercortisolism, manifested by typical phenotypic changes, severe secondary osteoporosis, and arterial hypertension in a young patient.
The diagnosis of Cushing’s syndrome is always challenging, given the presence of confounding factors such as the following:
Frequent and, even unknown, short- and long-term use of corticosteroids under different presentations;
Increase in the general population incidence of diabetes and obesity;
Screening tests with singularities for collection and individualized for different patient profiles.
It is important to note that the basal morning cortisol measurement is not the ideal test to assess hypercortisolism and is better applied to the assessment of adrenal insufficiency. However, the hypercortisolism of the case was unequivocal, and this test was also shown to be altered several times. As no test is 100% accurate, the current guidelines suggest the use of at least two first-line functional tests that focus on different aspects of the pathophysiology of the hypothalamic‒pituitary‒adrenal axis to confirm the hypercortisolism state: 24-hours cortisol, nocturnal salivary cortisol, morning serum cortisol after suppression with 1 mg of dexamethasone or after Liddle 1. Given that night-time salivary cortisol would require hospitalization, the other suggested tests were chosen, which are easier to perform in this context [7, 8].
Subsequently, tests were performed to determine the cause of hypercortisolism, such as serum ACTH levels and adrenal CT. The suppressed ACTH denoted the independence of its action. CT showed bilateral adrenal nodules with more severe features: solid lesion, attenuation > 10 UI on noncontrast images, and contrast washout speed < 60% in 10 minutes. In this case, it is essential to make a broad clinical decision and dialog with the patient to weigh and understand the risks and benefits of surgical treatment [9].
Among the main diagnostic hypotheses for the differential diagnosis of bilateral adrenal hyperplasia are primary bilateral macronodular adrenal hyperplasia, McCune–Albright syndrome (MAS) and bilateral primary pigmented nodular hyperplasia (PPNAD) isolated or associated with Carney’s complex. Another possibility would be bilateral adrenocorticotropic hormone (ACTH)-dependent macronodular hyperplasia secondary to long-term adrenal stimulation in patients with Cushing’s disease (ACTH-secreting pituitary tumor) or ectopic ACTH production, but the present case did not present with ACTH elevation.
Primary macronodular adrenal hyperplasia (nodules > 1 cm) predominates in women aged 50–60 years and may also be detected in early childhood (before 5 years) in the context of McCune–Albright syndrome. Most cases are considered sporadic; however, there are now several reports of familial cases whose presentation suggests autosomal dominant transmission. Several pathogenic molecular causes were identified in the table, indicating that it is a heterogeneous disease [10]. The pathophysiology occurs through the expression of anomalous ectopic hormone receptors or amplified eutopic receptors in the adrenals. It usually manifests in an insidious and subclinical way, with cortisol secretion mediated through receptors for gastric inhibitory peptide (GIP), vasopressin (ADH), catecholamines, interleukin 1 (IL-1), leptin, luteinizing hormone (LH), serotonin or others. Nodular development is not always synchronous or multiple; thus, hypercortisolism only manifests when there is a considerable increase in the number of adrenocortical cells, with severe steroidogenesis observed by cortisoluria greater than 3 times the upper limit of normal. Patients with mild Cushing’s syndrome should undergo screening protocols to identify aberrant receptors, as this may alter the therapeutic strategy. If there is evidence of abnormal receptors, treatment with beta-blockers is suggested for patients with beta-adrenergic receptors or with gonadotropin-releasing hormone (GnRH) agonists (and sex steroid replacement) for patients with LH/hCG receptors. In patients in whom aberrant hormone receptors are not present or for whom no specific pharmacological blockade is available or effective, the definitive treatment is bilateral adrenalectomy, which is known to make the patient dependent on chronic corticosteroid therapy [11]. Studies have shown the effectiveness of unilateral surgery in the medium and long term, opting for the resection of the adrenal gland of greater volume and nodularity by CT, regardless of the values obtained by catheterization of adrenal veins, but with the possibility of persistence or recurrence in the contralateral gland. Another possibility would be total unilateral adrenalectomy associated with subtotal contralateral adrenalectomy [12].
In McCune–Albright syndrome (MAS), there are activating mutations in the G-protein GNAS1 gene, generating autonomic hyperfunction of several tissues, endocrine or not, and there may be, for example, a constant stimulus similar to ACTH on the adrenal gland. In this case, pituitary levels of ACTH are suppressed, and adrenal adenomas with Cushing’s syndrome appear. Hypercortisolism may occur as an isolated manifestation of the syndrome or be associated with the triad composed of polyostotic fibrous dysplasia, café au lait spots with irregular borders and gonadal hyperfunction with peripheral precocious puberty. The natural history of Cushing’s syndrome in McCune-Albright syndrome (MAS) is heterogeneous, with some children evolving with spontaneous resolution of hypercortisolism, while others have a more severe condition, eventually requiring bilateral adrenalectomy [13].
PPNAD predominates in females, in people younger than 30 years, multiple and small (< 6 mm) bilateral pigmented nodules (surrounded by atrophied cortex), which can reach 1.5 cm in adulthood, with family genetic inheritance (66%) or sporadic inheritance (33%), and as part of the Carney complex reported in 40% of cases. In 70% of cases, inactivating mutations are identified in the PKA regulatory 1-alpha subunit (PRKAR1A), a tumor suppressor gene [14]. Osteoporosis is often associated with this condition [15]. One test that can distinguish patients with PPNAD from other primary adrenocortical lesions is cortisoluria after sequential suppression with low- and high-dose dexamethasone. In contrast to most patients with primary adrenocortical disease, who demonstrate no change in urinary cortisol, 70% of PPNAD patients have a paradoxical increase in urinary cortisol excretion [16]. The treatment of choice for PPNAD is bilateral adrenalectomy due to the high recurrence rate for primary adrenal disease [17].
Carney complex is a multiple neoplastic syndrome with autosomal dominant transmission, characterized by freckle-like cutaneous hyperpigmentation (lentiginosis), endocrine tumors [(PPNAD), testicular and/or thyroid tumors and acromegaly] and nonendocrine tumors, including cutaneous, cardiac, mammary, and osteochondral myxomas, among others. In the above case, the transthoracic echocardiogram of the patient on 03/18/2021 showed cavities of normal dimensions, preserved systolic and diastolic functions, no valve changes and no lentiginous skin areas and blue nevi, making the diagnosis of the syndrome less likely. The definitive diagnosis of Carney requires two or more main manifestations. Several related clinical components may suggest the diagnosis but not define it. The diagnosis can also be made if a key criterion is present and a first-degree relative has Carney or an inactivating mutation of the gene encoding PRKAR1A [18].
The adenoma is usually small in size (< 3 cm), similar to the nodules in this case; however, it is usually unilateral, with an insidious and mild evolution, especially in adult women over 35 years of age, producing only 1 steroid class. Carcinomas are usually large (> 6 cm), and only 10% are bilateral. They should be suspected mainly when the tumor presents with hypercortisolism associated with hyperandrogenism. They have a bimodal age distribution, with peaks in childhood and adolescence, as well as at the end of life [3].
Conclusion
Early identification of Cushing’s syndrome, with measures based on the assessment of risks and benefits, remains the best way to prevent progression and reduce morbidity [2]. After 6 months of drug inhibition of steroidogenesis, blood pressure control and anti-osteoporotic therapy, the objective was to minimize the levels and deleterious metabolic effects of hypercortisolism, which could also harm the surgical procedure in the short and long term through infections, dehiscence, nonimmediate bed mobilization and cardiovascular events. Unilateral adrenalectomy was chosen, given the possibility of malignancy in a young patient and to avoid definitive surgical adrenal insufficiency if the adrenalectomy was bilateral. Despite the unavailability of genetic analysis for a precise etiological definition, it is possible to take efficient measures to avoid unnecessary consequences or damage.
Pedro AO, Plapler PG, Szejnfeld VL. Manual brasileiro de osteoporose: orientações práticas para os profissionais de saúde. 1st ed. São Paulo: Editora Clannad; 2021. ISBN 978-65-89832-00-3.
Naguib R, Elkemary EZ, Elsharkawi KM. The severity of bone loss: a comparison between Cushing’s disease and Cushing’s syndrome. J Endocrinol Metab. 2023;13(1):33–8. https://doi.org/10.14740/jem857.
Wang D, Dang CX, Hao YX, Yu X, Liu PF, Li JS. Relationship between osteoporosis and Cushing syndrome based on bioinformatics. Medicine (Baltimore). 2022;101(43): e31283.
Williams TA, Reincke M. Management of Endocrine Disease: diagnosis and management of primary aldosteronism: the Endocrine Society guideline 2016 revisited. Eur J Endocrinol. 2018;179(1):R19–29. https://doi.org/10.1530/EJE-17-0990.
Compston J, Cooper A, Cooper C, Gittoes N, Gregson C, Harvey N, National Osteoporosis Guideline Group (NOGG), et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos. 2017;12(1):43. https://doi.org/10.1007/s11657-017-0324-5.
Hsiao HP, Kirschner LS, Bourdeau I, Keil MF, Boikos SA, Verma S, et al. Clinical and genetic heterogeneity, overlap with other tumor syndromes, and atypical glucocorticoid hormone secretion in adrenocorticotropin-independent macronodular adrenal hyperplasia compared with other adrenocortical tumors. J Clin Endocrinol Metab. 2009;94(8):2930–7. https://doi.org/10.1210/jc.2009-0516.
Stratakis CA, Sarlis N, Kirschner LS, Carney JA, Doppman JL, Nieman LK, et al. Paradoxical response to dexamethasone in the diagnosis of primary pigmented nodular adrenocortical disease. Ann Intern Med. 1999;131(8):585–91. https://doi.org/10.7326/0003-4819-131-8-199910190-00006.
Almeida MQ, Stratakis CA. Carney complex and other conditions associated with micronodular adrenal hyperplasias. Best Pract Res Clin Endocrinol Metab. 2010;24(6):907–14. https://doi.org/10.1016/j.beem.2010.10.006.
Serviço de Endocrinologia, Hospital Universitário da Universidade Federal de Juiz de Fora, Juiz de Fora, Minas Gerais, Brazil
Bárbara Oliveira Reis, Christianne Toledo Sousa Leal, Danielle Guedes Andrade Ezequiel, Ana Carmen dos Santos Ribeiro Simões Juliano, Flávia Lopes de Macedo Veloso, Leila Marcia da Silva, Lize Vargas Ferreira, Mariana Ferreira & Gabriel Zeferino De Oliveira Souza
Contributions
All the authors contributed to the conception and design of the work and have approved the submitted version. All authors read and approved the final manuscript.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Surgical removal of adrenal gland.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
RSS Error: A feed could not be found at `http://www.oconnormusic.org/feed.xml`; the status code is `503` and content-type is `text/html; charset=us-ascii`
RSS Error: A feed could not be found at `http://www.oconnormusic.org/bios.xml`; the status code is `503` and content-type is `text/html; charset=us-ascii`





")



-and-placenta-(D)")
-and-standard-deviation-(SD)")
-bilateral-multilobar-pneumonia")
-depicting-an-8x8-cm-hematoma-(arrow)-involving-the-left-psoas-and-iliacus-muscles")
-of-the-brain-depicting-a-1.3x1.3x3.2-cm-pituitary-macroadenoma-(star)")


From https://www.cureus.com/articles/243881-unveiling-the-uncommon-cushings-syndrome-cs-masquerading-as-severe-hypokalemia#!/