You may have heard of so-called ‘adrenal fatigue,’ supposedly caused by ongoing emotional stress. Or you might have come across adrenal support supplements sold online to treat it. But if someone suggests you have the controversial, unproven condition, seek a second opinion, experts say. And if someone tries to sell you dietary supplements or other treatments for adrenal fatigue, be safe and save your money.
Physicians tend to talk about ‘reaching’ or ‘making’ a medical diagnosis. However, when it comes to adrenal fatigue, endocrinologists – doctors who specialize in diseases involving hormone-secreting glands like the adrenals – sometimes use language such as ‘perpetrating a diagnosis,’ ‘misdiagnosis,’ ‘made-up diagnosis,’ ‘a fallacy’ and ‘nonsense.’
About 20 years ago, the term “adrenal fatigue” was coined by Dr. James Wilson, a chiropractor. Since then, certain practitioners and marketers have promoted the notion that chronic stress somehow slows or shuts down the adrenal glands, causing excessive fatigue.
“The phenomenon emerged from the world of integrative medicine and naturopathic medicine,” says Dr. James Findling, a professor of medicine and director of the Community Endocrinology Center and Clinics at the Medical College of Wisconsin. “It has no scientific basis, and there’s no merit to it as a clinical diagnosis.”
An online search of medical billing code sets in the latest version of the International Classification of Diseases, or the ICD-10, does not yield a diagnostic code for ‘adrenal fatigue’ among the 331 diagnoses related either to fatigue or adrenal conditions or procedures.
In a March 2020 position statement, the American Association of Clinical Endocrinologists and American College of Endocrinology addressed the use of adrenal supplements “to treat common nonspecific symptoms due to ‘adrenal fatigue,’ an entity that has not been recognized as a legitimate diagnosis.”
The position statement warned of known and unknown health risks of off-label use and misuse of hormones and supplements in patients without an established endocrine diagnosis, as well as unnecessary costs to patients and the overall health care system.
Study after study has refuted the legitimacy of adrenal fatigue as a medical diagnosis. An August 2016 systematic review combined and analyzed data from 58 studies on adrenal fatigue including more than 10,000 participants. The conclusion in a nutshell: “Adrenal fatigue does not exist,” according to review authors in the journal BMC Endocrine Disorders.
Adrenal Action
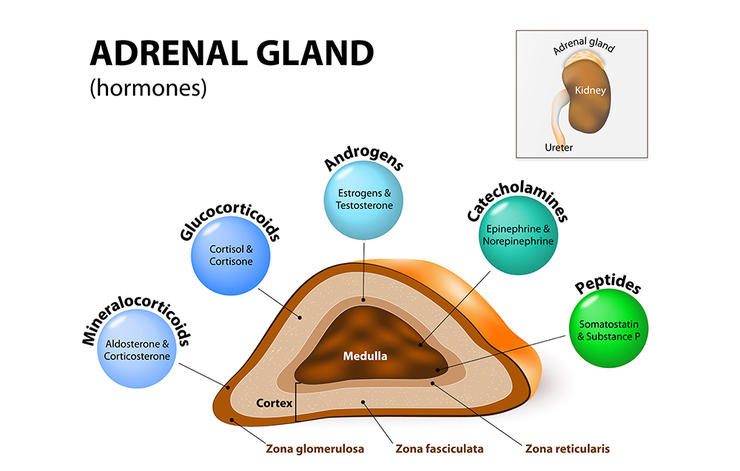
You have two adrenal glands in your body. These small triangular glands, one on top of each kidney, produce essential hormones such as aldosterone, cortisol and male sex hormones such as DHEA and testosterone.
Cortisol helps regulate metabolism: How your body uses fat, protein and carbohydrates from food, and cortisol increases blood sugar as needed. It also plays a role in controlling blood pressure, preventing inflammation and regulating your sleep/wake cycle.
As your body responds to stress, cortisol increases. This response starts with signals between two sections in the brain: The hypothalamus and the pituitary gland, which act together to release a hormone that stimulates the adrenal glands to make cortisol. This interactive unit is called the hypothalamic pituitary adrenal axis.
While some health conditions really do affect the body’s cortisol-making ability, adrenal fatigue isn’t among them.
“There’s no evidence to support that adrenal fatigue is an actual medical condition,” says Dr. Mary Vouyiouklis Kellis, a staff endocrinologist at Cleveland Clinic. “There’s no stress connection in the sense that someone’s adrenal glands will all of a sudden just stop producing cortisol because they’re so inundated with emotional stress.”
If anything, adrenal glands are workhorses that rise to the occasion when chronic stress occurs. “The last thing in the body that’s going to fatigue are your adrenal glands,” says Dr. William F. Young Jr., an endocrinology clinical professor and professor of medicine in the Mayo Clinic College of Medicine at Mayo Clinic in Rochester, Minnesota. “Adrenal glands are built for stress – that’s what they do. Adrenal glands don’t fatigue. This is made up – it’s a fallacy.”
The idea of adrenal glands crumbling under stress is “ridiculous,” Findling agrees. “In reality, if you take a person and subject them to chronic stress, the adrenal glands don’t shut down at all,” Findling says. “They keep making cortisol – it’s a stress hormone. In fact, the adrenal glands are just like the Energizer Bunny – they just keep going. They don’t stop.”
Home cortisol tests that allow consumers to check their own levels can be misleading, Findling says. “Some providers who make this (adrenal fatigue) diagnosis, provide patients with testing equipment for doing saliva cortisol levels throughout the day,” he says. “And then, regardless of what the results are, they perpetrate this diagnosis of adrenal fatigue.”
Saliva cortisol is a legitimate test that’s frequently used in diagnosing Cushing’s syndrome, or overactive adrenal glands, Findling notes. However, he says, a practitioner pursuing an adrenal fatigue diagnosis could game the system. “What they do is: They shape a very narrow normal range, so narrow, in fact, that no normal human subject could have all their saliva cortisol (levels) within that range throughout the course of the day,” he says. “Then they convince the poor patients that they have adrenal fatigue phenomena and put them on some kind of adrenal support.”
Loaded Supplements
How do you know what you’re actually getting if you buy a dietary supplement marketed for adrenal fatigue or ‘adrenal support’ use? To find out, researchers purchased 12 such supplements over the counter in the U.S.
Laboratory tests revealed that all supplements contained a small amount of thyroid hormone and most contained at least one steroid hormone, according to the study published in the March 2018 issue of Mayo Clinic Proceedings. “These results may highlight potential risks for hidden ingredients in unregulated supplements,” the authors concluded.
Supplements containing thyroid hormones or steroids can interact with a patient’s prescribed medications or have other side effects.
“Some people just assume they have adrenal fatigue because they looked it up online when they felt tired and they ultimately buy these over-the-counter supplements that can be very dangerous at times,” Vouyiouklis Kellis says. “Some of them contain animal (ingredients), like bovine adrenal extract. That can suppress the pituitary axis. So, as a result, your body stops making its own cortisol or starts making less of it, and as a result, you can actually worsen the condition rather than make it better.”
Any form of steroid from outside the body, whether a prescription drug like prednisone or extract from cows’ adrenal glands, “can shut off the pituitary,” Vouyiouklis Kellis explains. “Because it’s signaling to the pituitary like: Hey, you don’t need to stimulate the adrenals to make cortisol, because this patient is taking it already. So, as a result, the body ultimately doesn’t produce as much. And, so, if you rapidly withdraw that steroid or just all of a sudden decide not to take it anymore, then you can have this acute response of low cortisol.”
Some adrenal support products, such as herbal-only supplements, may be harmless. However, they’re unlikely to relieve chronic fatigue.
Fatigue: No Easy Answers
If you’re suffering from ongoing fatigue, it’s frustrating. And you’re not alone. “I have fatigue,” Young Jr. says. “Go to the lobby any given day and say, ‘Raise your hand if you have fatigue.’ Most of the people are going to raise their hands. It’s a common human symptom and people would like an easy answer for it. Usually there’s not an easy answer. I think ‘adrenal fatigue’ is attractive because it’s like: Aha, here’s the answer.”
There aren’t that many causes of endocrine-related fatigue, Young Jr. notes. “Hypothyroidism – when the thyroid gland is not working – is one.” Addison’s disease, or adrenal insufficiency, can also lead to fatigue among a variety of other symptoms. Established adrenal conditions – like adrenal insufficiency – need to be treated.
“In adrenal insufficiency, there is an intrinsic problem in the adrenal gland’s inability to produce cortisol,” Vouyiouklis Kellis explains. “That can either be a primary problem in the adrenal gland or an issue with the pituitary gland not being able to stimulate the adrenal to make cortisol.”
Issues can arise even with necessary medications. “For example, very commonly, people are put on steroids for various reasons: allergies, ear, nose and throat problems,” Vouyiouklis Kellis says. “And with the withdrawal of the steroids, they can ultimately have adrenal insufficiency, or decrease in cortisol.”
Opioid medications for pain also result in adrenal sufficiency, Vouyiouklis Kellis says, adding that this particular side effect is rarely discussed. People with a history of autoimmune disease can also be at higher risk for adrenal insufficiency.
Common symptoms of adrenal insufficiency include:
- Fatigue.
- Weight loss.
- Decreased appetite.
- Salt cravings.
- Low blood pressure.
- Abdominal pain.
- Nausea, vomiting or diarrhea.
- Muscle weakness.
- Hyperpigmentation (darkening of the skin).
- Irritability.
Medical tests for adrenal insufficiency start with blood cortisol levels, and tests for the ACTH hormone that stimulates the pituitary gland.
“If the person does not have adrenal insufficiency and they’re still fatigued, it’s important to get to the bottom of it,” Vouyiouklis Kellis says. Untreated sleep apnea often turns out to be the actual cause, she notes.
“It’s very important to tease out what’s going on,” Vouyiouklis Kellis emphasizes. “It can be multifactorial – multiple things contributing to the patient’s feeling of fatigue.” The blood condition anemia – a lack of healthy red blood cells – is another potential cause.
“If you are fatigued, do not treat yourself,” Vouyiouklis Kellis says. “Please seek a physician or a primary care provider for evaluation, because you don’t want to go misdiagnosed or undiagnosed. It’s very important to rule out actual causes that would be contributing to symptoms rather than ordering supplements online or seeking an alternative route like self-treating rather than being evaluated first.”