Cushing’s syndrome patients with tumors on both adrenal glands — which sit on top of the kidneys — could undergo adrenal venous sampling, a procedure where blood samples are taken from both adrenal glands to determine which tumors to remove, researchers suggest.
Their study, “Outcomes of Adrenal Venous Sampling in Patients with Bilateral Adrenal Masses and ACTH-Independent Cushing’s Syndrome,” was published in the World Journal of Surgery. The work was a collaboration between SUNY Upstate Medical University in Syracuse and the University of Pittsburgh.
Cushing’s syndrome, a condition characterized by excess cortisol, can be divided into two main subtypes. In some patients, the disease is dependent on tumors secreting the adrenocorticotropic hormone (ACTH), which stimulates the release of cortisol from the adrenal glands. In others, adrenal tumors are solely responsible for excess cortisol and do not require ACTH for functioning.
ACTH-independent Cushing’s syndrome (AICS), the latter subtype, constitutes about 10% to 15% of endogenous — an overproduction of cortisol within the body — Cushing’s syndrome cases, with cortisol-secreting adenomas in just one gland (unilateral) being the most common cause.
Compared to unilateral adenomas, adrenal tumors in both glands (bilateral) in patients with AICS are difficult to diagnose. Disease management in these rare cases depends on the challenging determination of the lesion’s exact location and of the functional status of the benign tumors (if they are actively secreting cortisol).
Surgical removal of both adrenal glands, also known as bilateral adrenalectomy, “ensures cure of AICS, but leads to permanent corticosteroid dependence and a lifelong risk of adrenal crisis,” investigators explained. Therefore, screening for the presence of unilateral or bilateral adenomas is essential to avoid unnecessary surgery.
“Adrenal venous sampling (AVS) has been reported in a single institutional series … to aid in successful localization of cortisol-secreting adrenal adenomas in patients with bilateral adrenal masses and AICS,” researchers wrote.
Researchers retrospectively assessed the usefulness of AVS in guiding management of patients with bilateral adrenal masses plus AICS.
Nine women (age 51-73) with bilateral adrenal masses and AICS were included in the study. All subjects had undergone AVS at the University of Pittsburgh Medical Center from 2008 to 2016. None of the patients had apparent symptoms of Cushing’s syndrome.
“Samples were obtained for testing of epinephrine [also called adrenaline] and cortisol from both [adrenal veins] and the external iliac vein. Multiple samples were obtained to ensure adequate sampling,” they wrote.
Adrenal glands produce cortisol and epinephrine, among other hormones, which are critical for maintaining good health. In AICS, there’s an overproduction of both hormones that’s independent on the release of ACTH, which is produced by the brain’s pituitary gland.
Successful adrenal venous sampling was achieved in eight women. “One patient with unsuccessful catheterization had [other additional diseases] and passed away from unrelated reasons,” researchers reported.
AVS results indicated that all patients had bilateral cortisol-secreting adenomas.
“Surgical management was strongly influenced by adrenal mass size. However, AVS may have influenced surgical decision-making in some cases, particularly when minimal difference in size was noted in adrenal mass sizes,” they reported.
Six women underwent adrenalectomy: three had the gland with larger size mass removed (unilateral type of surgery); two had both glands removed; and one had the right gland removed followed by the left one, five months later, due to continuous hormonal overproduction without experiencing symptoms of Cushing’s syndrome.
Evidence suggests that removal of the larger adrenal mass in patients with bilateral cortisol-secreting adenomas improves Cushing’s syndrome presentation.
In theory, unilateral adrenalectomy reduces cortisol production through the removal of the oversecreting mass. Because of this, unilateral adrenalectomy of the larger adrenal mass was chosen in half of this study’s surgical cases, instead of bilateral adrenalectomy.
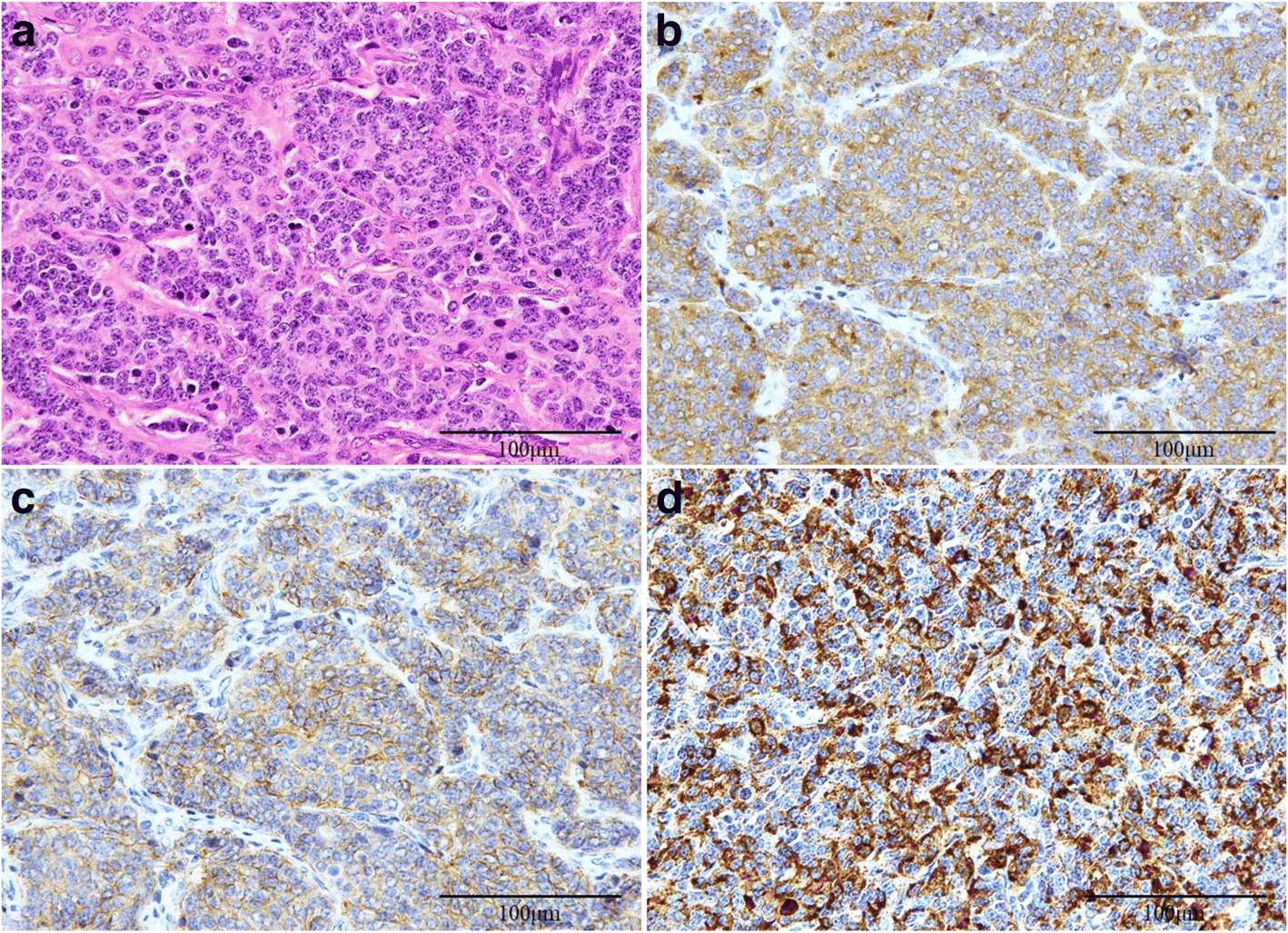
Tissue analysis revealed multiple-lump masses, also known as macronodular adrenal hyperplasia (MAH), in all six surgical cases.
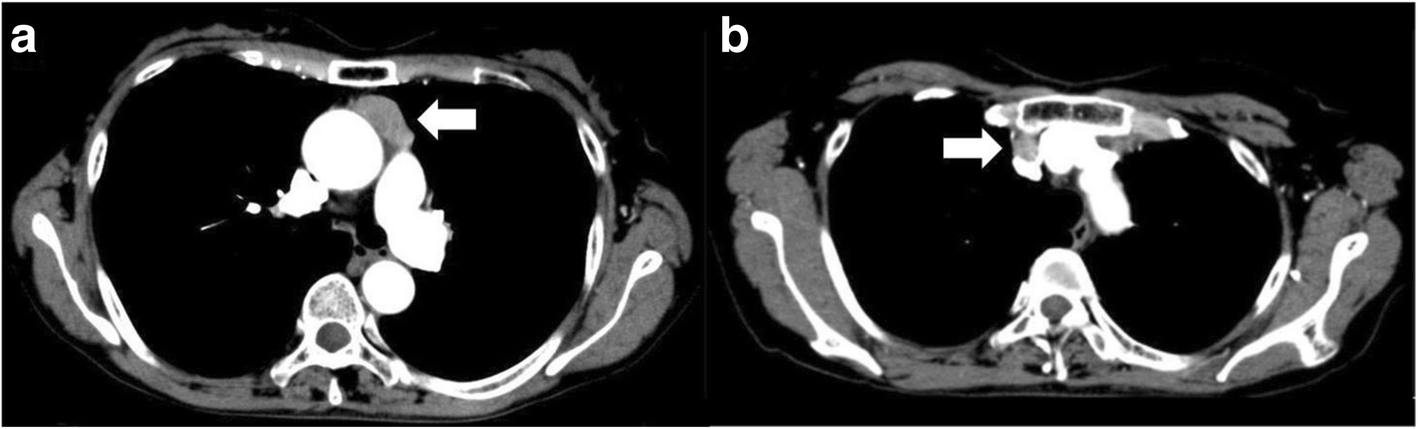
In addition, computed tomography (CT) scan findings were predictive of bilateral MAH, with scans showing evidence of one or multiple nodules on one or both adrenal glands.
“To the best of our knowledge, this is the second study to evaluate the utility of AVS in guiding management of patients with bilateral adrenal masses and AICS,” investigators said.
The first study was by Young and included 10 patients with a more severe presentation of Cushing’s syndrome and other individual characteristics, which contributed to the differences in results, compared to the current study. In Young’s study, half the subjects had unilateral adrenal masses.
Patients with bilateral cortisol-secreting masses frequently have a milder form of Cushing’s syndrome, which corroborates researchers’ findings.
Despite suggesting that adrenal venous sampling is useful in excluding a unilateral adenoma as the cause of AICS, this study’s sample size is small.
“More data are needed before AVS can be advocated as essential for management of patients with bilateral adrenal masses and AICS,” researchers concluded.
Filed under: adrenal, Cushing's, Treatments | Tagged: adrenal glands, adrenalectomy, Cushing's Syndrome | Leave a comment »