


The resection of microadenomas — small, benign tumors in the pituitary gland underlying Cushing’s disease — could be aided by a fluorescent marker that is naturally produced by the tumor, a new study shows.
The findings were presented recently at the 2018 George Washington Research Days in a poster titled, “Enhanced 5-ALA Induced Fluorescence in Hormone Secreting Pituitary Adenomas.”
Cushing’s disease is characterized by high cortisol levels that cause debilitating physical, mental, and hormonal symptoms. The excess cortisol is caused by tiny benign tumors in the pituitary gland, called microadenomas, with a size of less than 10 millimeters.
On account of their small size, these microadenomas pose imaging challenges to physicians. Up to 40 percent of microadenomas remain undetected in the gold-standard magnetic resonance imaging (MRI).
Pituitary adenomas, however, have a characteristic that distinguishes them from the surrounding healthy tissue. They process (metabolize) a natural haemoglobin metabolite, called 5-aminolevulinic acid (5-ALA), into protoporphyrin IX (PpIX) at much higher rates — up to 20 to 50 times higher — than normal tissues.
Importantly, PpIX emits red fluorescence when excited with blue light.
This means that exogenous 5-ALA is taken up by the adenoma cells and rapidly metabolized into the fluorescent metabolite, PpIX, which may establish its use for fluorescence-guided resection of pituitary adenomas.
To test this, researchers incubated human-derived corticotropinoma, as well as the adjacent normal gland cells with 5-ALA. They did the same with mouse model normal pituitary cells and a mouse model pituitary tumor cell line, called AtT20.
They then analyzed the cells’ fluorescence profile by microscopy and with a technique called flow cytometry.
The analysis showed that compared to normal pituitary tissue, human-derived adenomatous cells had a significant increase of tenfold in 5-ALA-induced PpIX fluorescence intensity.
Similarly, mouse pituitary tumor cells (AtT20 cell line) fluoresced seven times more intensely than normal murine pituitary tissue.
The microscopy analysis revealed that the 5-ALA localized in subcellular organelles called mitochondria.
On June 6, 2017, the U.S. Food and Drug Administration approved the use of 5-ALA (under the brand name Gleolan) as an optical imaging agent for patients with gliomas (brain tumors), as an add-on compound to assist surgeons in identifying the malignant tissue during surgery.
Now, these findings suggest that 5-ALA also may be used for fluorescence-guided surgery of microadenomas in Cushing’s disease.
“The supraphysiological levels of glucocorticoids, as seen in CD [Cushing’s disease], may enhance the 5-ALA fluorescence in corticotropinomas,” researchers wrote.
Filed under: Cushing's, pituitary, Treatments | Tagged: 2018 George Washington Research Days, 5-ALA, 5-aminolevulinic acid (5-ALA), corticotropinomas, Cushing's Disease, fluorescent marker, Gleolan, hemoglobin, MRI, pituitary tumors, PpIX, protoporphyrin IX (PpIX), surgery | Leave a comment »
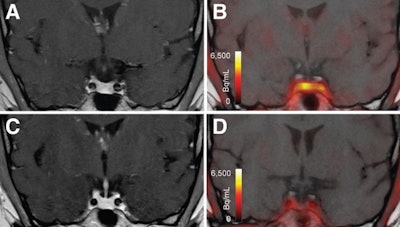 T1-weighted postgadolinium MR images (A and C) and F-18 FET-PET/MR images (B and D) centered at pituitary before (A and B) and after (C and D) transsphenoidal surgery. This patient with Cushing disease showed clear focal uptake (B) but no clear lesion on previously obtained and accompanying MRI (A). Postoperative tissue analysis did confirm resection of small pituitary adenoma/PitNET, and postoperative F-18 FET-PET showed no residual uptake (D). Image courtesy of the Journal of Nuclear Medicine.
T1-weighted postgadolinium MR images (A and C) and F-18 FET-PET/MR images (B and D) centered at pituitary before (A and B) and after (C and D) transsphenoidal surgery. This patient with Cushing disease showed clear focal uptake (B) but no clear lesion on previously obtained and accompanying MRI (A). Postoperative tissue analysis did confirm resection of small pituitary adenoma/PitNET, and postoperative F-18 FET-PET showed no residual uptake (D). Image courtesy of the Journal of Nuclear Medicine.