Doctors should suspect Cushing’s syndrome when they see patients with purple stretch marks and metabolic conditions such as diabetes, even if those symptoms aren’t the reasons for a medical visit, physicians in Japan wrote in a case study describing how they reached that diagnosis for a woman in her early 30s.
To assess coronary inflammation by measuring the volume and density of the epicardial adipose tissue (EAT), perivascular fat attenuation index (FAI) and coronary plaque burden in patients with Cushing’s syndrome (CS) based on coronary computed tomography angiography (CCTA).
Methods
This study included 29 patients with CS and 58 matched patients without CS who underwent CCTA. The EAT volume, EAT density, FAI and coronary plaque burden were measured. The high-risk plaque (HRP) was also evaluated. CS duration from diagnosis, 24-h urinary free cortisol (UFC), and abdominal visceral adipose tissue volume (VAT) of CS patients were recorded.
Results
The CS group had higher EAT volume (146.9 [115.4, 184.2] vs. 119.6 [69.0, 147.1] mL, P = 0.006), lower EAT density (− 78.79 ± 5.89 vs. − 75.98 ± 6.03 HU, P = 0.042), lower FAI (− 84.0 ± 8.92 vs. − 79.40 ± 10.04 HU, P = 0.038), higher total plaque volume (88.81 [36.26, 522.5] vs. 44.45 [0, 198.16] mL, P = 0.010) and more HRP plaques (7.3% vs. 1.8%, P = 0.026) than the controls. The multivariate analysis suggested that CS itself (β [95% CI], 29.233 [10.436, 48.03], P = 0.014), CS duration (β [95% CI], 0.176 [0.185, 4.242], P = 0.033), and UFC (β [95% CI], 0.197 [1.803, 19.719], P = 0.019) were strongly associated with EAT volume but not EAT density, and EAT volume (β [95% CI] − 0.037[− 0.058, − 0.016], P = 0.001) not CS was strongly associated with EAT density. EAT volume, FAI and plaque burden increased (all P < 0.05) in 6 CS patients with follow-up CCTA. The EAT volume had a moderate correlation with abdominal VAT volume (r = 0.526, P = 0.008) in CS patients.
Conclusions
Patients with CS have higher EAT volume and coronary plaque burden but less inflammation as detected by EAT density and FAI. The EAT density is associated with EAT volume but not CS itself.
Cushing’s syndrome (CS) secondary to adrenocorticotropic hormone (ACTH) producing tumours is a severe condition with a challenging diagnosis. Ectopic ACTH-secretion often involves neuroendocrine tumours (NET) in the respiratory tract.
ACTH-secreting small intestine neuro-endocrine tumours (siNET) are extremely rare entities barely reported in literature. This review is illustrated by the case of a 75-year old woman with fulminant ectopic CS caused by a ACTH-secreting metastatic siNET. Severe hypokalemia, fluid retention and refractory hypertension were the presenting symptoms. Basal and dynamic laboratory studies were diagnostic for ACTH-dependent CS.
Phaeochromocytoma with ectopic ACTH secretion. Its clinical presentation is varied, and diagnosis is challenging.
Ectopic ACTH secretion from a phaeochromocytoma can rapidly progress to severe Cushing’s syndrome.
Removal of the primary tumour often leads to full recovery.
Abstract
Introduction
The occurrence of hypercortisolism resulting from adrenocorticotropic hormone (ACTH)-secreting pheochromocytoma is exceedingly uncommon, with limited documented instances thus far.
Presentation of case
We present a case of ectopic ACTH-secreting pheochromocytoma in a patient who suffered from severe metabolic disorders. Our clinical case outlines the diagnostic history, preoperative correction of the patient’s metabolic disturbances and surgical strategy for management of a rare ectopic ACTH producing pheochromocytoma.
Discussion
Ectopic adrenocorticotropic hormone-secreting pheochromocytoma displays multifaceted clinical features and requires prompt diagnosis and multidisciplinary management in order to overcome the related severe clinical derangements.
Conclusion
The combination of biochemical and hormonal testing and imaging procedures is mandatory for the diagnosis of ectopic ACTH secretion, and in the presence of an adrenal mass, the possibility of an ACTH-secreting pheochromocytoma should be taken into account.
Neuroendocrine tumors such as Pheochromocytoma and paraganglioma (PPGL) are an uncommon occurrence. The prevalence of PPGL has been estimated to be between (2–8)/1 million, with a population rate of 1:2500–1:6500 [1], and it is associated with symptoms such as headache, irregular heartbeats, profuse sweating, high blood pressure, nausea, vomiting, nervousness, irritability, and a sense of imminent mortality [2]. Hypercortisolism is also a rare disorder with an incidence of 5/1 million, <10 % of patients with hypercortisolism are caused by ectopic secretion of ACTH [3], and these are most commonly seen in APUD tumors such as small cell bronchopulmonary carcinoma, pancreatic islet carcinoma, medullary thyroid carcinoma, pheochromocytoma, and melanoma [4]. Tumors that secrete both ACTH and catecholamines are much rarer. Here, we present a case of ectopic ACTH-secreting pheochromocytoma with severe metabolic disorders. The case report is compliant with SCARE Guidelines [5].
2. Case report
The patient is a 46-year-old male who presented to our hospital with recurrent symptoms of pheochromocytoma. He reported that he experienced unexplained symptoms such as panic attacks, headache, sweating, nausea, vomiting, and a feeling of imminent death, which could be alleviated by rest. His blood pressure was around 160–220/110–120 mmHg, and he was taking oral antihypertensive drugs regularly, with poor control of his blood pressure. The patient was admitted with a body temperature of 36.7 °C, heart rate of 130 beats/min, respiratory rate of 20 cycles per minute, blood pressure of 138/88 mmHg, height of 175 cm, weight of 67 kg, Body Mass Index (BMI): 21.88, normal physical examination, emaciated body type, thin subcutaneous fat, self-reported weight loss of 20 kg within 10 months, and history of diabetes mellitus of >1 year.
Laboratory tests showed that the blood potassium levels were within the normal range, while the blood sugar and beta-hydroxybutyrate levels were elevated (Table 1). Hormonal analysis showed plasma levels of free catecholamine and its metabolites were much higher than normal, in addition to a severe excess of cortisol secretion with circadian rhythm disorders and elevated serum ACTH (Table 2). Small dose dexamethasone suppression test (1 mg) yielded cortisol levels of over 1750 nmol/L (negative: no decrease in blood cortisol), thus confirming the presence of ACTH-dependent hypercortisolism. The results of electrocardiogram, chest computerized tomography (CT), cardiac ultrasound and thyroid ultrasound showed no obvious abnormality. Enhanced CT of the adrenal glands (Fig. 1) revealed the presence of a right adrenal tumor measuring approximately 5.3 ∗ 4.7 cm. Despite undergoing cranial MRI, no pituitary lesion was detected, thereby ruling out the possibility of Cushing’s disease. The patient was further considered for possible ectopic ACTH syndrome and suspected ectopic ACTH-secreting pheochromocytoma.
Fig. 1. Adrenal CT showed a 53 ∗ 47 mm mass in the right adrenal gland.
In response to the patient’s pheochromocytoma symptoms and improve preoperative preparation, we used α-blocker (Phenoxybenzamine 20 mg q8h) to lower blood pressure and increase blood volume, antihypertensive medication (nifedipine 30 mg q12h, olmesartan tablets 20 mg q12h) to assist in lowering blood pressure, and β-blocker (metoprolol 47.5 mg q12h) to control the heart rate. On the 4th day in hospital, the patient was lethargic and had weak limbs. Urgent blood workup showed severe hypokalemia (2.85 mmol/L) as well as hyperglycemia (10.26 mmol/L). Patient was transferred to intensive care to correct intractable hypokalemia and diabetic ketoacidosis.
After the patient was transferred to ICU, a deep vein cannulation was performed with intravenous potassium chloride supplementation, and the patient’s blood potassium was maintained at normal levels prior to surgery through a large amount of potassium supplementation (Fig. 2A). For diabetic ketoacidosis, insulin administration, rehydration, ketone elimination and other treatments were given and the amount of access was recorded, and it was found that the patient was polyuric, with the highest urine volume of 21,800 ml in a single day (Fig. 2B), and the amount of urine did not decrease by taking oral desmopressin tablets 0.1 mg bid.
Fig. 2. Changes in blood potassium and urine volume during the patient’s hospitalization. A: Blood potassium level. B: Daily urine vlume.
Eventually, the patient underwent laproscopic right adrenal tumor resection. Intraoperative changes in blood pressure and heart rate are shown in Fig. 3. On day 1 after surgery, the morning (8:00) ACTH level was 10.60 pg/ml, antihypertensive medications were discontinued, and his blood pressure was 100–120/60–90 mmHg. The patient’s daily urine output and blood glucose gradually returned to normal levels after surgery. Pathology (Fig. 4): Adrenal pheochromocytoma with ACTH immunopositive staining, cellular heterogeneity was unremarkable, nuclear schizophrenic images were rare, no pericytes, choroidal invasion and necrosis were seen. The patient was discharged from the clinic in a satisfactory condition with adrenal insufficiency compensated by daily intake of Prednisone Acetate Tablets (20 mg), discontinued 6 months after surgery. No signs of recurrence were noted upon frequent follow-up examinations.
Fig. 4. Immunohistochemistry. A: hematoxylin and eosin staining B: ACTH.
3. Discussion
We share the management of a patient with ectopic ACTH-secreting pheochromocytoma with severe metabolic disturbances, where, in addition to the rare etiology, perioperative management of the clinical complications of catecholamines and hypercortisolism is very challenging [6].
Patients suffering from ectopic ACTH syndrome caused by pheochromocytoma commonly exhibit severe Cushing’s syndrome (CS), significant diabetes mellitus, hypertension, and hypokalemia [7]. Additionally, a retrospective study revealed that the majority of patients presented with Cushing’s syndrome [8], whereas another report indicated that only 30 % of patients presented with typical Cushing’s syndrome, but weight loss was frequently observed [9]. Our patient’s recent weight loss may be attributed to the body’s hypermetabolic condition caused by catecholamines. Recent reports claim that catecholamines directly reduce subcutaneous and visceral fat [10]. Rapid onset of cortisolism appears to be a feature of ACTH-secreting pheochromocytomas, because of the rapid onset of severe hypercortisolism, and our patient did not exhibit typical Cushing’s symptoms [8].
Despite the absence of typical Cushing-like symptoms, this patient displayed persistent hypokalemia, a prevalent metabolic manifestation of Cushing’s syndrome, particularly in ectopic ACTH syndrome, where hypokalemia is observed in 74 %–95 % of patients, in contrast to 10 % of patients with Cushing’s disease [11]. Glucocorticoids have the ability to interact with aldosterone receptors, resulting in specific aldosterone-like reactions, while ectopic ACTH syndrome typically generates a higher amount of cortisol compared to Cushing’s disease, ultimately causing more pronounced hypokalemia [7]. The perioperative management of patients with ACTH-secreting pheochromocytomas poses a significant challenge due to severe hypokalemia, and our patient’s potassium levels remained within the normal range through extensive central venous potassium supplementation, without the need for cortisol secretion inhibition medications.
The severity of hypertension in patients with ACTH-secreting pheochromocytomas seems to surpass that of patients with pheochromocytomas alone [12]. Hypercortisolism amplifies catecholamine-induced hypertension [13]. In the case of hypertension in patients with pheochromocytomas, alpha-blockers are favored for reducing blood pressure and enlarging blood volume, while for individuals whose blood pressure is not adequately managed with alpha-blockers alone, a combination of medications is recommended. Proper preoperative readiness for expanding the volume is crucial for a successful surgical procedure. Patients with ACTH-secreting pheochromocytoma have a greater prevalence and intensity of diabetes mellitus compared to those with pheochromocytoma alone [14], and our patient displayed a combination of severe diabetes mellitus and ketoacidosis. Insulin exhibits swift action and adaptable dosage, effectively averting hypoglycemia and effectively addressing hyperglycemia, rendering it the preferred medication for regulating blood glucose levels in individuals with ectopic CS [6].
Managing the water-electrolyte balance in this patient proved to be an arduous task, and the diabetes insipidus may have been one of the complications, with a maximum urine output of 21,800 ml in a single day (Fig. 2), and we hold the belief that the patient’s diabetes insipidus is caused by a range of factors, such as hypokalemia, hypercortisolism, and severe diabetes mellitus. Indeed, hypokalemia may cause renal impairment, which reduces the ability to concentrate urine and lack of response to antidiuretic hormone (ADH), leading to nephrogenic diabetes insipidus [15]. Cortisol increases renal plasma flow and glomerular filtration rate, and also inhibits the secretion of antidiuretic hormone, leading to neurogenic diabetes insipidus [16].
For hypercortisolism, surgery to target the cause is the first-line treatment, and surgical removal of primary tumor may lead to 40 % radical treatment and 80 % complete remission of ectopic ACTH syndrome [17].
4. Conclusion
Preoperative diagnosis and management of pheochromocytoma, an extremely rare cause of ectopic ACTH syndrome, is challenging. Proper preoperative recognition of complications of both hypercortisolism and catecholamines excess is the key to prevent the morbidity and mortality of an ACTH-producing pheochromocytoma. If diagnosed successfully and managed intensively, they are curable.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Shandong Provincial Hospital Affiliated to Shandong First Medical University does not require ethical approval for publication of case reports. Signed consent from the patient has been received.
Funding
No funding was received for this research.
Author contribution
Shangjian Li: study concept or design, data collection, data analysis or interpretation, writing the paper
Xudong Guo: study concept or design, data collection, data analysis or interpretation, writing the paper
Hanbo Wang: study concept or design, data analysis or interpretation
Ni Suo: study concept or design, data analysis or interpretation
Xiuqing Mi: study concept,data collection
Shaobo Jiang: study concept or design, data analysis or interpretation, writing the paper
M.F. Birtolo, E.M. Grossrubatscher, S. Antonini, et al.
Preoperative management of patients with ectopic Cushing’s syndrome caused by ACTH-secreting pheochromocytoma: a case series and review of the literature
J. Endocrinol. Investig., 46 (2023), pp. 1983-1994
Case report of severe Cushing’s syndrome in medullary thyroid cancer complicated by functional diabetes insipidus, aortic dissection, jejunal intussusception, and paraneoplastic dysautonomia: remission with sorafenib without reduction in cortisol concentration
Patients with Cushing’s disease (CD) face challenges living with and receiving appropriate care for this rare, chronic condition. Even with successful treatment, many patients experience ongoing symptoms and impaired quality of life (QoL). Different perspectives and expectations between patients and healthcare providers (HCPs) may also impair well-being.
Objective
To examine differences in perspectives on living with CD between patients and HCPs, and to compare care goals and unmet needs.
Design
Memorial Sloan Kettering Pituitary Center established an annual pituitary symposium for pituitary patients and HCPs. Through anonymous pre-program surveys distributed at the 2020 and 2022 symposia, patients and HCPs answered questions related to their own sense, or perception of their patients’ sense, of hope, choice, and loneliness in the context of living with CD.
Participants
From 655 participants over two educational events, 46 patients with CD and 116 HCPs were included. Median age of both groups was 51 years. 78.3% of the patients were female vs. 53.0% of the HCPs.
Results
More patients than HCPs reported they had no choices in their treatment (21.7% vs. 0.9%, P < 0.001). More patients reported feeling alone living with CD than HCPs’ perception of such (60.9% vs. 45.5%, P = 0.08). The most common personal care goal concern for patients was ‘QoL/mental health,’ vs. ‘medical therapies/tumor control’ for HCPs. The most common CD unmet need reported by patients was ‘education/awareness’ vs. ‘medical therapies/tumor control’ for HCPs.
Conclusions
CD patients experience long term symptoms and impaired QoL which may in part be due to a perception of lack of effective treatment options and little hope for improvement. Communicating experiences and care goals may improve long term outcomes for CD patients.
Introduction
Patients with rare diseases face challenges receiving appropriate care. Cushing’s disease (CD), a condition associated with excess endogenous glucocorticoids due to an ACTH-secreting pituitary tumor, is a rare disease, occurring in 0.7 to 2.4 per million per year [1]. Patients with CD are at high risk for metabolic, cardiovascular, and psychiatric disease, in addition to long-term symptom burden and impaired quality of life (QoL), despite adequate treatment [1,2,3].
A critical aspect of effective patient care is communication and mutual understanding between healthcare provider (HCP) and patient. Patients with pituitary tumors experience significant anxiety associated with their diagnosis, in large part due to difficulties interacting with healthcare systems and limited communication of information [4]. Many pituitary patients express concern regarding the complexity of their care, and satisfaction improves with the delivery of more information by the HCP [4]. Patients with pituitary tumors, and CD specifically, require multidisciplinary care which necessitates effective communication in order to provide the best possible outcomes [5].
Similar to acromegaly patients [6], CD patients’ long-term well-being may be adversely affected by different perspectives and expectations between patients and HCPs, especially after treatment [7]. While HCPs primarily use biochemical data to define successful treatment, patients rely more on their symptoms and ability to regain normal functioning [7]. Despite achieving biochemical remission, CD patient perception of having persistent disease negatively impacts QoL [8]. In addition, 67.5% of Cushing’s syndrome patients report receiving insufficient information from their HCPs regarding the recovery experience after surgery despite the fact that all HCPs report providing this information [9]. Improved communication between HCPs and CD patients is vital to optimizing patients’ QoL and long term outcomes.
Recently there has been a growing emphasis on the use of internet-based platforms for healthcare delivery and education [10]. With the goals of offering HCP and patient education and assessing pituitary patients’ needs, since 2019 the pituitary center at Memorial Sloan Kettering (MSK) has offered annual virtual educational programs for pituitary patients, caregivers, HCPs, and members of the pharmaceutical industry. For the current study, we gathered deidentified information from 2020 to 2022 MSK program participants on CD patients’ and HCPs’ attitudes about CD, related to their sense of hope, choice, and loneliness, through anonymous pre-program surveys. Our specific aims were to: (1) Assess differences in perspectives between patients’ and HCPs’ responses in the pre-program survey; (2) Compare patients’ and HCPs’ perceived care goals and unmet needs.
Methods
Educational program enrollment
The MSK program was offered to patients with any type of pituitary tumor as well as HCPs, family members, caregivers, and members of industry. The role of the registrant as a patient, caregiver/family member, HCP, and/or member of industry was determined for all registrants of the virtual programs.
Any patient with a pituitary tumor treated at our center and outside institutions, inclusive of patients at all points along their treatment journey, were invited to register for the virtual education program. HCPs, including endocrinologists, neurosurgeons, otolaryngologists, radiation oncologists, neurologists, ophthalmologists, neuro-oncologists, family medicine and internal medicine physicians, physicians in training and other allied health professionals who treat and manage patients with pituitary diseases were also invited to register. Invitations were sent through email to neuroendocrine experts and endocrinologists, patient support groups on social media, direct messaging to patients with pituitary tumors by their treating physicians and via patient databases, advertisements through endocrine societies, brochure/postcard mailing, and Eventbrite, a virtual platform for live events.
Study participants
Registrants from MSK virtual programs held on December 5, 2020, (n = 328) and April 9, 2022, (n = 327) were included in the pool of subjects, among which the qualifying participants were determined.
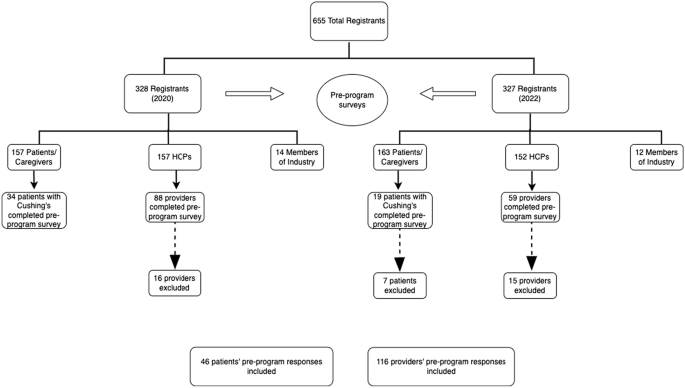
Of the 655 total registrants from the 2020 and 2022 programs, 320 (48.9%) were patients or caregivers and 309 (47.2%) were HCPs (Fig. 1). Of the 147 providers (88 in 2020 and 59 in 2022) that attended and filled out a pre-program survey 31 were excluded from our analysis. Eight filled out surveys in both 2020 and 2022, 4 were members of industry, 3 did not fill out any responses, and 1 was not in the healthcare field. In addition, 12 providers had at least three fields missing in the survey and 3 had filled out two surveys for the same year, so they were also excluded. A total of 116 providers (72 from 2020 to 44 from 2022) were included in the analysis.
Among the 320 pituitary patients who attended the programs (157 from 2020 to 163 from 2022), 53 identified as ‘patients with Cushing’s’ and submitted surveys (34 participants from 2020 to 19 from 2022). Seven patients were excluded from the 2022 surveys as they had also filled out surveys in 2020, leaving a final group of 46 patients who were included in the analysis.
Virtual education programs
For each program, there was a single day of live interactive programming, meaning that all participants attended at the same time. The programs were recorded and made available for several weeks as enduring material for registrants on an online website.
After joint sessions in the morning, both programs consisted of two tracks in the afternoon: the ‘provider/clinical track’ and the ‘patient/caregiver track’. During the programs, an ongoing chat reeled through the virtual program which allowed patients to continually ask questions. Faculty experts answered these questions in written responses directly within the chat and/or in spoken responses during one of the live broadcasted Q&A sessions. Additionally, the programs both included panel discussions answering patient questions and moderated patient discussions with invited patient speakers.
Study procedures
Through anonymous pre-program surveys distributed at the 2020 and 2022 symposia, patients and HCPs answered questions related to their own sense, or perception of their patients’ sense, of hope, choice, and loneliness in the context of living with CD. This survey was developed by a multidisciplinary team and has been reported previously [11]. Demographic and clinical information was also assessed including year of diagnosis, prior treatments, and current medications (for patients) and specialty and practice type (for providers), as shown in Tables 1 and 2. Multiple-choice questions assessing patients’ attitudes toward their disease included possible answers of ‘I have no hope for improvement,’ ‘I have some hope for improvement,’ and ‘I have a lot of hope for improvement;’ and ‘I have no choice in my treatment,’ ‘I have some choices in my treatment,’ and ‘I have many choices in my treatment.’ Patients were also asked to respond ‘TRUE’ or ‘FALSE’ to the following statements: ‘I feel alone living with my Cushing’s,’ ‘Hearing the journeys of other patients helps me better understand my own,’ and ‘I feel anxious about my Cushing’s diagnosis.’
Multiple-choice questions assessing providers’ attitudes about their patients’ Cushing’s included possible answers of ‘I have no hope for their improvement,’ ‘I have some hope for their improvement,’ and ‘I have a lot of hope for their improvement;’ and ‘my patients have no choice in their treatment,’ ‘my patients have some choices in their treatment,’ and ‘my patients have many choices in their treatment.’ Providers were also asked to respond ‘TRUE’ or ‘FALSE’ to the following statements: ‘my patients feel alone living with their Cushing’s,’ ‘Hearing the journeys of other patients helps will help my patients better understand their own,’ and ‘my patients feel anxious about their Cushing’s diagnosis.’
Additionally, patients were surveyed on care goals and unmet needs related to their treatment. Specifically, patients were asked, ‘What are the healthcare outcomes/goals that matter to you the most?’ and ‘What do you think are unmet needs for the diagnosis or treatment of your condition?’ The first question was intended to refer to the patient specifically, while the second question was meant to examine how the condition is treated in general. Survey responses were submitted as free text and subsequently grouped by the authors (AH and EBG) into nine different categories: (a) Quality of life (QoL)/Mental Health; (b) Medical Therapies/Tumor Control; (c) Education/Awareness; (d) Communications/Multidisciplinary Care; (e) Insurance/Access; (f) Fertility; (g) Controlling Comorbidities; (h) Support System and (i) none. Responses could receive multiple designations if applicable. AH coded the free text themes independently, then EBG reviewed each answer and corresponding grouping to confirm accuracy. If there was disagreement or confusion, coding from our prior work [11] was reviewed.
HCPs were also surveyed on care goals and unmet needs related to their patient’s treatment. Providers were asked, ‘What are the healthcare outcomes/goals that matter to you the most?’ and ‘what do you think are unmet needs for the diagnosis or treatment of your patient’s condition?’ The first question was intended to refer to the provider and their goals related to Cushing’s, while the second question was meant to examine how the condition is treated in general. Survey responses were submitted as free text and subsequently grouped by the authors (AH and EBG) into nine different categories: (a) Quality of life (QoL)/Mental Health; (b) Medical Therapies/Tumor Control; (c) Education/Awareness; (d) Communications/Multidisciplinary Care; (e) Insurance/Access; (f) Fertility; (g) Controlling Comorbidities; (h) Support System and (i) none. Responses could receive multiple designations if applicable.
Statistical analysis
Descriptive statistics were presented as counts and percentages for categorical variables and as medians and interquartile range (IQR) for continuous variables. The Chi-square test or Fisher’s exact test was used to compare gender and survey responses between the CD patient group and the HCP group. All statistical tests were two-tailed, and a P-value of < 0.05 was considered statistically significant. SAS Software® (version 9.4; SAS Institute Inc., Cary, NC) was used for all analyses.
Results
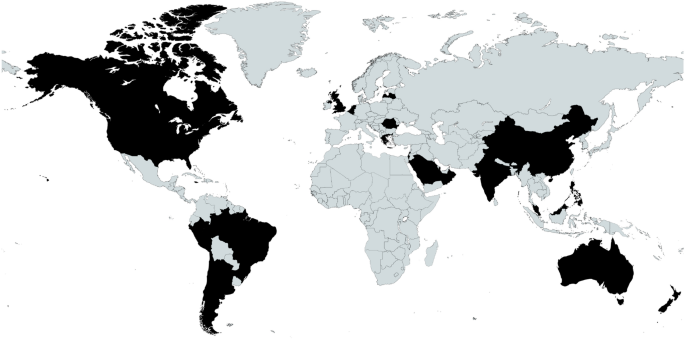
Between the 2020 and 2022 events, there was combined representation from 25 different countries. A map and a full list of the countries is shown in Fig. 2.
Fig. 2
Map of registrant locations. Locations (listed alphabetically): Argentina, Australia, Belgium, Brazil, Canada, Chile, China, Greece, Hong Kong, India, Israel, Jamaica, Latvia, Malaysia, Netherlands, New, Zealand, Oman, Peru, Philippines, Qatar, Romania, Saudi Arabia, Singapore, UK, US
From a total of 655 participants over two educational events, 46 patients with CD and 116 HCP caring for CD patients were included in the analysis. The demographic data of the patients and HCPs are outlined in Tables 1 and 2, respectively. Median age of the patients and HCPs was 51 years. 78.3% of the CD group was female vs. 53.0% of the HCP group (P = 0.003).
CD patients ranged from newly diagnosed to being diagnosed 33 years prior. The HCPs who filled out the pre-program surveys were in practice for a mean duration of 18.5 years, with a range from 1 to 54 years.
As shown in Table 1, CD patients had a mean duration of suspected active disease prior to diagnosis of 5.26 years, as defined by onset of CD symptoms until diagnosis, and a mean duration of disease since diagnosis of 5.9 years. 42 (91%) had undergone surgical treatment of their Cushing’s. For those who underwent surgery, the mean number of surgeries was 1.17 (range 0–4). 20% had received pituitary radiation. Overall, 31% of patients were on medical therapy for Cushing’s. Metyrapone was the most used CD therapy (in 11%), followed by ketoconazole (in 9%). Of those requiring pituitary hormone replacement, 34.8% had one pituitary hormone deficiency and 21.7% had multiple hormone deficiencies. Thyroid hormone replacement (37%) and adrenal replacement (30%) were the most common.
As shown in Table 2, the majority of the HCPs were endocrinologists (72%) followed by neurosurgeons (9%) and nurses (8%). There was a total of 9 different specialties represented by the provider group. 16% of the providers worked in private practice, 16% were hospital based, and 16% worked in ‘unspecified clinical care.’ 38% of the providers practice type was ‘unspecified.’
Based on the pre-program survey responses, we identified different attitudes between patients and HCPs in several domains. Table 3 depicts pre-program survey responses from CD patients and HCPs assessing their attitudes about CD. 21.7% of patients reported they had no choices in their treatment, compared to 0.9% of HCPs (P < 0.001). Almost all HCPs (99.1%) reported that CD patients had least some choice in their management. In addition, less than half (45.7%) of patients reported they had a lot of hope for improvement whereas 71.3% of HCPs had a lot of hope for their patients’ improvement. Surprisingly, fewer CD patients reported feeling anxious about their diagnosis compared to HCPs’ perceived patient anxiety (65.2% vs 94.6%, P < 0.001). However, more patients tended to feel more alone living with CD than HCPs’ perception of such (60.9% vs. 45.5%, P = 0.08). Both CD patients and HCPs agreed that hearing the journeys of other CD patients would help patients better understand their own disease (97.8% vs 100%).
Table 3 Patient and provider attitudes by pre-program survey
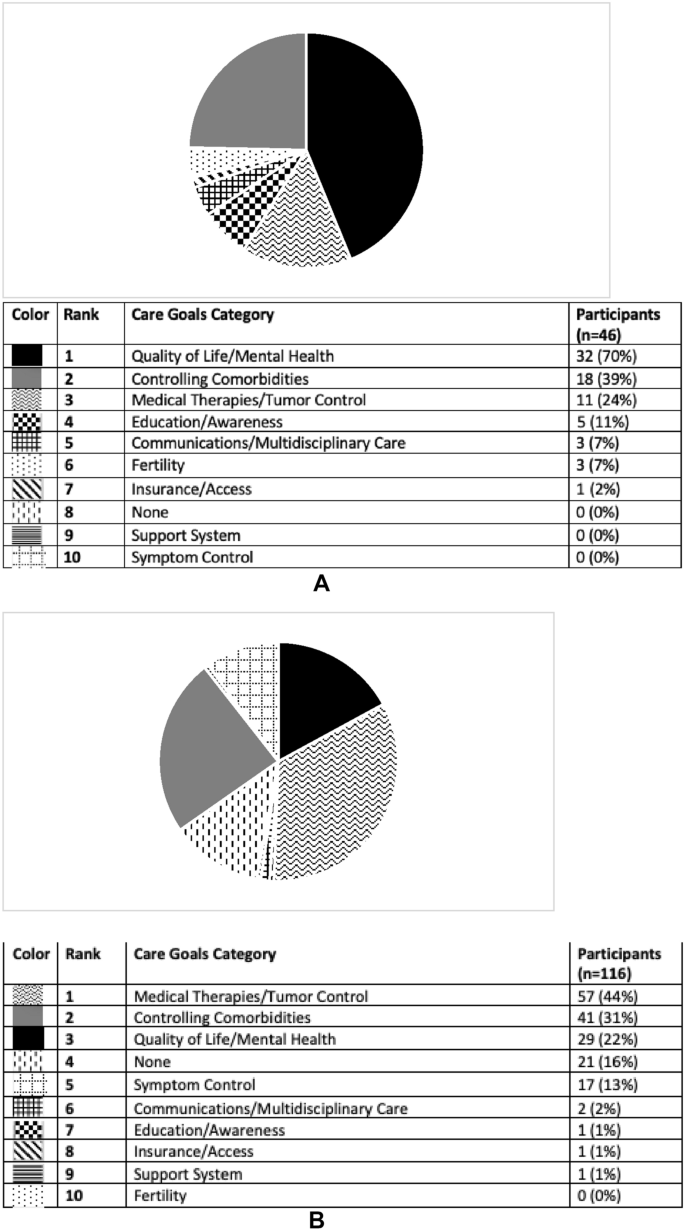
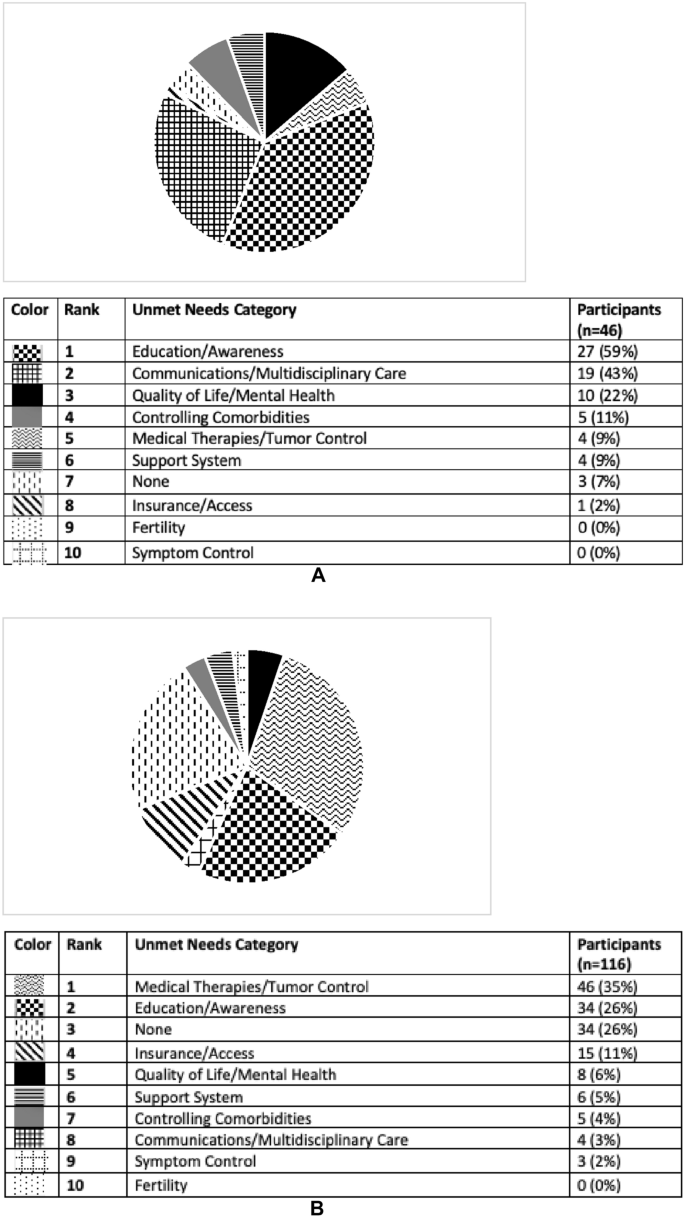
CD patients and HCPs were also surveyed on their personal care goals and unmet needs, results of which are shown in Figs. 3A, B and 4A, B. The most common personal care goal concern for patients was ‘QoL/mental health’ which was reported by 70%, followed by ‘controlling comorbidities’ (39%) and ‘medical therapies/tumor control’ (24%). HCPs prioritized the same three care goals as patients but ‘medical therapies/tumor control’ was the most common (44%). ‘Controlling comorbidities’ and ‘QoL/mental health’ were the second and third most often HCP reported care goals (31 and 22% respectively). ‘Education/awareness’ was the most common perceived CD unmet need by patients (59%). HCPs reported both ‘medical therapies/tumor control’ and ‘education/awareness’ to be the most common unmet needs (35 and 26%, respectively). Examples of patient and provider responses, and how they were coded, are shown in Supplemental Table 1.
Fig. 3
A Care goals according to participants with Cushing’s who completed pre-program survey. This pie graph represents the free-text survey response from patients regarding their personal care goals as categorized by topic. B Care goals according to providers who completed pre-program survey. This pie graph represents the free-text survey response from providers regarding their personal care goals as categorized by topic
A Unmet needs for the field of Cushing’s disease according to participants with Cushing’s who completed pre-program survey. This pie graph represents the free-text survey response from patients regarding unmet needs in Cushing’s as categorized by topic. B Unmet needs for the field of Cushing’s disease according to providers who completed pre-program survey. This pie graph represents the free-text survey response from providers regarding unmet needs in Cushing’s as categorized by topic
This study examined the differences between patients and HCP-reported perceptions of living with CD. We identified several differences in disease outlook between CD patients and HCPs. We found that more patients than HCPs reported they had no choices in their treatment. Furthermore, less than half of patients reported they had a lot of hope for improvement whereas most (71.3%) of HCPs had a lot of hope for their patients’ improvement. Interestingly, fewer CD patients reported feeling anxious about their diagnosis compared to HCPs’ perceived patient anxiety, although a higher percentage of patients reported feeling alone living with CD compared to the HCPs’ perception of patient loneliness. We also identified HCP and patient differences in reported personal care goals and perceived unmet needs in the field. The most common personal care goal concern for patients was ‘QoL/mental health,’ whereas it was ‘medical therapies/tumor control’ for HCPs. ‘Education/awareness’ was the most commonly perceived unmet need by patients, whereas it was ‘medical therapies/tumor control’ for HCPs.
Our findings support prior work demonstrating a discrepancy between patients and HCPs regarding the need for improved multidisciplinary care [12]. 43% of patients listed ‘communication/multidisciplinary care’ as an unmet need in the field, compared to 3% of providers. Pituitary centers of excellence provide expert multidisciplinary care in the neuroendocrine, neurosurgical, and radiation oncology domains, but often lack expertise in mental and physical health domains salient for CD patients, who suffer from depression, anxiety, myopathy and joint pain. In order to offer comprehensive care, psychiatrists, psychologists, social workers, pain medicine experts, physical therapists, and nutritionists with expertise in CD should be included in the pituitary center multidisciplinary team [13]. Our findings suggest that pituitary centers of excellence should take into account the most important personal care goal reported by CD patients, which is Qol/mental health, and provide expert treatment in this domain.
It is not surprising that Qol/mental health is the personal care goal most reported by CD patients. Prior assessment of acromegaly patients demonstrated the same finding: QoL/mental health was the most common personal care goal concern [11]. While surgical [14] and medical [15,16,17,18] treatment of Cushing’s improves QoL, QoL has been shown to remain impaired over time after treatment [19]. Several factors may contribute to long-term Qol impairments, including the presence of persistent disease, imperfect treatment modalities which themselves may be associated with burden and adverse side effects, and persistent comorbidities including depression, anxiety, fatigue, and overweight. Perception of disease status may also play a role in QoL. In surgically remitted CD patients, there may be discordance between biochemical remission and perceived disease status [8]. Specifically, this study found that of those with self-identified persistence of disease, 65% were in fact biochemically remitted. This group had lower QoL scores than the concordant group who self-identified as in remission with biochemical evidence of remission.
CD patients’ outlook on their condition, including their perception of choices and hope for change, has not been previously well described, despite the fact that these perceptions likely inform long term Qol. Patient outlook may be a modifiable target that if addressed, could improve long term patient well-being and outcomes. Aside from continuing progress in the development of new therapies for CD patients which can offer patients more objective choices in their treatment, other modalities should be considered. Prior work has shown that virtual educational programs improve acromegaly patients’ hope for improvement, perception of having choices in their treatment, and sense of loneliness [11]. Educational programs have also been shown to result in improved physical activity and sleep, and reduced pain levels in CS patients [20]. More work is needed to develop effective education programming tailored for CD patients to provide the appropriate support that these patients need.
Difference in HCP and patient disease perceptions may also play a role in Cushing’s patients’ quality of life and outcomes. Among a cohort of patients who underwent surgical resection for Cushing’s, 32.4% reported not receiving information from their doctors about the recovery experience, despite the fact that all physicians surveyed reported giving information about the recovery process [9]. Furthermore, 16.1% of patients in this cohort reported that not enough medical professionals were familiar with the symptoms of Cushing’s. Recovery time was also reported to be longer by patients than providers [9]. Similarly, discordance was found between acromegaly patients and HCPs regarding reported severity of symptoms, with patients more frequently reporting symptoms as severe compared to HCPs, and many patients reporting symptoms which were not reported by HCPs [6]. Improving communication between HCP and patients may positively affect CD patient outlook and QoL.
We identified a similar disparity between CD patients and HCP regarding care goals and unmet needs. 70% of patients surveyed considered QoL/mental health to be a top care goal, but only 22% of provider shared this goal. 59% of patients reported education/awareness as an unmet need, compared to 26% of HCPs. These findings support data shown by Acre et al. in which Cushing’s patients report a lack of symptom recognition by their providers [9]. HCPs should be aware that their patients may have different treatment priorities.
Our finding that more HCPs reported patient anxiety living with CD compared to patients themselves needs further exploration. This could reflect inadequate communication between HCP and patient, or skewed HCP perceptions of CD. This, and other findings in our study should be viewed in light of the small cohort, and as such, needs confirmation in larger cohorts and more in-depth symptom assessments. Additional limitations of our study include lack of paired patient-HCP responses as the HCPs included were not providing care for this specific CD cohort. Since this was a pituitary educational forum, likely most or all patients who identified as having Cushing’s had CD. However, our survey did not specify the type of surgery patients underwent or the etiology of their Cushing’s. Additionally, we used multidisciplinary team agreed upon measures and not validated assessments. Further work should consider validating a tool to assess patient-provider discordances. Our findings may also be confounded by selection bias, given that the patients participating in our virtual education programs are more likely to be under the care of experts in the field and may not represent the attitudes of all patients living with CD. Finally, the included HCPs were representatives from a range of specialties with different levels of experience taking care of patients with CD which may also affect their responses.
Our findings highlight the importance of understanding CD patients’ outlook and perspective in their condition, and that they may differ from their HCP. More than half of CD patients did not have a lot of hope for improvement and reported feeling alone, and many patients felt they had no choices in their treatment. QOL/mental health was the most commonly reported care goal for patients, which was not the case for HCPs. Comprehensive multidisciplinary care for CD patients should include mental health professionals with expertise in CD. Regular open communication between HCPs and CD patients will help bridge perception differences and facilitate personalized care, which will ultimately improve long-term outcomes for CD patients.
Data availability
The data that support the findings of this study are available from the authors upon request.
Kreitschmann-Andermahr I, Siegel S, Gammel C et al (2018) Support needs of patients with Cushing’s disease and Cushing’s syndrome: results of a survey conducted in Germany and the USA. Int J Endocrinol 2018:9014768. https://doi.org/10.1155/2018/9014768
Feelders RA, Pulgar SJ, Kempel A, Pereira AM (2012) The burden of Cushing’s disease: clinical and health-related quality of life aspects. Eur J Endocrinol 167(3):311–326. https://doi.org/10.1530/EJE-11-1095
Donegan D, Gowan T, Gruber R et al (2021) The need for patient-centered education among patients newly diagnosed with a pituitary tumor. J Endocr Soc. https://doi.org/10.1210/jendso/bvab061
Geer EB, Sisco J, Adelman DT et al (2020) Observed discordance between outcomes reported by acromegaly patients and their treating endocrinology medical provider. Pituitary 23(2):140–148. https://doi.org/10.1007/s11102-019-01013-2
Carluccio A, Sundaram NK, Chablani S et al (2015) Predictors of quality of life in 102 patients with treated Cushing’s disease. Clin Endocrinol (Oxf) 82(3):404–411. https://doi.org/10.1111/cen.12521
Acree R, Miller CM, Abel BS, Neary NM, Campbell K, Nieman LK (2021) Patient and provider perspectives on postsurgical recovery of Cushing syndrome. J Endocr Soc. https://doi.org/10.1210/jendso/bvab109
Ca BM, Badiu C, Bonomi M et al (2017) Developing and evaluating rare disease educational materials co-created by expert clinicians and patients: the paradigm of congenital hypogonadotropic hypogonadism. Orphanet J Rare Dis 12(1):57. https://doi.org/10.1186/s13023-017-0608-2
Valassi E, Santos A, Yaneva M et al (2011) The European registry on Cushing’s syndrome: 2-year experience. Baseline demographic and clinical characteristics. Eur J Endocrinol 165(3):383–392. https://doi.org/10.1530/EJE-11-0272
Casanueva FF, Barkan AL, Buchfelder M et al (2017) Criteria for the definition of pituitary tumor centers of excellence (PTCOE): a pituitary society statement. Pituitary 20(5):489–498. https://doi.org/10.1007/s11102-017-0838-2
Santos A, Resmini E, Martinez-Momblan MA et al (2012) Psychometric performance of the Cushing QoL questionnaire in conditions of real clinical practice. Eur J Endocrinol 167(3):337–342. https://doi.org/10.1530/EJE-12-0325
Colao A, Petersenn S, Newell-Price J et al (2012) A 12-month phase 3 study of pasireotide in Cushing’s disease. N Engl J Med 366(10):914–924. https://doi.org/10.1056/NEJMoa1105743
Fleseriu M, Biller BM, Findling JW et al (2012) Mifepristone, a glucocorticoid receptor antagonist, produces clinical and metabolic benefits in patients with Cushing’s syndrome. J Clin Endocrinol Metab 97(6):2039–2049. https://doi.org/10.1210/jc.2011-3350
Geer EB, Salvatori R, Elenkova A et al (2021) Levoketoconazole improves clinical signs and symptoms and patient-reported outcomes in patients with Cushing’s syndrome. Pituitary 24(1):104–115. https://doi.org/10.1007/s11102-020-01103-6
Pivonello R, Fleseriu M, Newell-Price J et al (2020) Efficacy and safety of osilodrostat in patients with Cushing’s disease (LINC 3): a multicentre phase III study with a double-blind, randomised withdrawal phase. Lancet Diabetes Endocrinol 8(9):748–761. https://doi.org/10.1016/S2213-8587(20)30240-0
Page-Wilson G, Oak B, Silber A et al (2023) Evaluating the burden of endogenous Cushing’s syndrome using a web-based questionnaire and validated patient-reported outcome measures. Pituitary. https://doi.org/10.1007/s11102-023-01314-7
Martínez-Momblán MA, Gómez C, Santos A et al (2016) A specific nursing educational program in patients with Cushing’s syndrome. Endocrine 53:199–209. https://doi.org/10.1007/s12020-015-0737-0
The authors would like to thank the HCP and patient participants who attended the events, the MSK faculty, invited speakers, Leslie Edwin of Cushing’s Support and Research Foundation, Amy Edouard and the MSK CME team, and Recordati Rare Diseases, Inc., Amryt Pharma (previously Chiasma, Inc.), Crinetics, Sparrow Pharmaceuticals, Corcept Therapeutics, and Xeris Biopharma (previously Strongbridge Biopharma) for providing educational grants for these educational activities.
Funding
This research was funded in part through the NIH/NCI Cancer Center Support Grant P30 CA008748.
Author information
Authors and Affiliations
Division of Endocrinology, Department of Medicine, Weill Cornell Medicine, New York, NY, USA
Amanda Halstrom
Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, NY, USA
I.-Hsin Lin
Multidisciplinary Pituitary & Skull Base Tumor Center, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Andrew Lin, Marc Cohen, Viviane Tabar & Eliza B. Geer
Department of Neurology, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Andrew Lin
Department of Neurosurgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Andrew Lin, Marc Cohen & Eliza B. Geer
Head and Neck Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Marc Cohen & Viviane Tabar
Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Eliza B. Geer
Contributions
A.H. and E.B.G. wrote the manuscript text and prepared the figures. All authors reviewed the manuscript.
As an educational quality initiative project using de-identified data, it was determined that our project did not constitute human subjects research and thus did not require IRB oversight.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.