April is always Cushing’s Awareness Challenge month because Dr. Harvey Cushing was born on April 8th, 1869.
Thanks to Robin for this wonderful past logo! I’ve participated in these 30 days for Cushing’s Awareness several times so I’m not quite sure what is left to say this year but I always want to get the word out when I can.
As I see it, there have been some strides the diagnosis or treatment of Cushing’s since last year. More drug companies are getting involved, more doctors seem to be willing to test, a bit more awareness, maybe.
How fitting that this challenge should begin on April Fool’s Day. So much of Cushing’s Syndrome/Disease makes us Cushies seem like we’re the April Fool. Maybe, just maybe, it’s the doctors who are the April Fools…
Doctors tell us Cushing’s is too rare – you couldn’t possibly have it. April Fools!
All you have to do is exercise and diet. You’ll feel better. April Fools!
Those bruises on your legs? You’re just clumsy. April Fools!
Sorry you’re growing all that hair on your chin. That happens as you age, you know. April Fools!
Did you say you sleep all day? You’re just lazy. If you exercised more, you’d have more energy. April Fools!
You don’t have stretch marks. April Fools!
You have stretch marks but they are the wrong [color/length/direction] April Fools!
The hump on the back of your neck is from your poor posture. April Fools!
Your MRI didn’t show a tumor. You couldn’t have Cushing’s. April Fools!
This is all in your mind. Take this prescription for antidepressants and go home. April Fools!
If you have this one surgery, your life will get back to normal within a few months. April Fools!
What? You had transsphenoidal surgery for Cushing’s? You wasted your time and money. April Fools!
I am the doctor. I know everything. Do not try to find out any information online. You could not have Cushing’s. It’s too rare… April FOOL!
All this reminds me of a wonderful video a message board member posted a while ago:
So now – who is the April Fool? It wasn’t me. Don’t let it be you, either!
Transsphenoidal surgery — a minimally invasive surgery for removing pituitary tumors in Cushing’s disease patients — is also effective in children and adolescents with the condition, leading to remission with a low rate of complications, a study reports.
In the study, a team from Turkey shared its findings on 10 children and adolescents (7 females) with the condition, who underwent microsurgery (TSMS) or endoscopic surgery (ETSS, which is less invasive) — the two types of transsphenoidal surgery.
At the time of surgery, the patients’ mean age was 14.8 years, and they had been experiencing symptoms for a mean average of 24.2 months. All but one had gained weight, with a mean body mass index of 29.97.
Their symptoms included excessive body hair, high blood pressure, stretch marks, headaches, acne, “moon face,” and the absence of menstruation.
The patients were diagnosed with Cushing’s after their plasma cortisol levels were measured, and there was a lack of cortical level suppression after they took a low-dose suppression treatment. Measurements of their adrenocorticotropic (ACTH) hormone levels then revealed the cause of their disease was likely pituitary tumors.
Magnetic resonance imaging (MRI) scans, however, only enabled tumor localization in seven patients: three with a microadenoma (a tumor smaller than 10 millimeters), and four showed a macroadenoma.
CD diagnosis was confirmed by surgery and the presence of characteristic pituitary changes. The three patients with no sign of adenoma on their MRIs showed evidence of ACTH-containing adenomas on tissue evaluation.
Eight patients underwent TSMS, and 2 patients had ETSS, with no surgical complications. The patients were considered in remission if they showed clinical adrenal insufficiency and serum cortisol levels under 2.5 μg/dl 48 hours after surgery, or a cortisol level lower than 1.8 μg/dl with a low-dose dexamethasone suppression test at three months post-surgery. Restoration of normal plasma cortisol variation, eased symptoms, and no sign of adenoma in MRI were also requirements for remission.
Eight patients (80%) achieved remission, 4 of them after TSMS. Two patients underwent additional TSMS for remission. Also, 1 patient had ETSS twice after TSMS to gain remission, while another met the criteria after the first endoscopic surgery.
The data further showed that clinical recovery and normalized biochemical parameters were achieved after the initial operation in 5 patients (50%). Three patients (30%) were considered cured after additional operations.
The mean cortisol level decreased to 8.71 μg/dl post-surgery from 23.435 μg/dl pre-surgery. All patients were regularly evaluated in an outpatient clinic, with a mean follow-up period of 11 years.
Two patients showed pituitary insufficiency. Also, 2 had persistent hypocortisolism — too little cortisol — one of whom also had diabetes insipidus, a disorder that causes an imbalance of water in the body. Radiotherapy was not considered in any case.
“Transsphenoidal surgery remains the mainstay therapy for CD [Cushing’s disease] in pediatric patients as well as adults,” the scientists wrote. “It is an effective treatment option with low rate of complications.”
Patients with Cushing’s disease (CD) face challenges living with and receiving appropriate care for this rare, chronic condition. Even with successful treatment, many patients experience ongoing symptoms and impaired quality of life (QoL). Different perspectives and expectations between patients and healthcare providers (HCPs) may also impair well-being.
Objective
To examine differences in perspectives on living with CD between patients and HCPs, and to compare care goals and unmet needs.
Design
Memorial Sloan Kettering Pituitary Center established an annual pituitary symposium for pituitary patients and HCPs. Through anonymous pre-program surveys distributed at the 2020 and 2022 symposia, patients and HCPs answered questions related to their own sense, or perception of their patients’ sense, of hope, choice, and loneliness in the context of living with CD.
Participants
From 655 participants over two educational events, 46 patients with CD and 116 HCPs were included. Median age of both groups was 51 years. 78.3% of the patients were female vs. 53.0% of the HCPs.
Results
More patients than HCPs reported they had no choices in their treatment (21.7% vs. 0.9%, P < 0.001). More patients reported feeling alone living with CD than HCPs’ perception of such (60.9% vs. 45.5%, P = 0.08). The most common personal care goal concern for patients was ‘QoL/mental health,’ vs. ‘medical therapies/tumor control’ for HCPs. The most common CD unmet need reported by patients was ‘education/awareness’ vs. ‘medical therapies/tumor control’ for HCPs.
Conclusions
CD patients experience long term symptoms and impaired QoL which may in part be due to a perception of lack of effective treatment options and little hope for improvement. Communicating experiences and care goals may improve long term outcomes for CD patients.
Introduction
Patients with rare diseases face challenges receiving appropriate care. Cushing’s disease (CD), a condition associated with excess endogenous glucocorticoids due to an ACTH-secreting pituitary tumor, is a rare disease, occurring in 0.7 to 2.4 per million per year [1]. Patients with CD are at high risk for metabolic, cardiovascular, and psychiatric disease, in addition to long-term symptom burden and impaired quality of life (QoL), despite adequate treatment [1,2,3].
A critical aspect of effective patient care is communication and mutual understanding between healthcare provider (HCP) and patient. Patients with pituitary tumors experience significant anxiety associated with their diagnosis, in large part due to difficulties interacting with healthcare systems and limited communication of information [4]. Many pituitary patients express concern regarding the complexity of their care, and satisfaction improves with the delivery of more information by the HCP [4]. Patients with pituitary tumors, and CD specifically, require multidisciplinary care which necessitates effective communication in order to provide the best possible outcomes [5].
Similar to acromegaly patients [6], CD patients’ long-term well-being may be adversely affected by different perspectives and expectations between patients and HCPs, especially after treatment [7]. While HCPs primarily use biochemical data to define successful treatment, patients rely more on their symptoms and ability to regain normal functioning [7]. Despite achieving biochemical remission, CD patient perception of having persistent disease negatively impacts QoL [8]. In addition, 67.5% of Cushing’s syndrome patients report receiving insufficient information from their HCPs regarding the recovery experience after surgery despite the fact that all HCPs report providing this information [9]. Improved communication between HCPs and CD patients is vital to optimizing patients’ QoL and long term outcomes.
Recently there has been a growing emphasis on the use of internet-based platforms for healthcare delivery and education [10]. With the goals of offering HCP and patient education and assessing pituitary patients’ needs, since 2019 the pituitary center at Memorial Sloan Kettering (MSK) has offered annual virtual educational programs for pituitary patients, caregivers, HCPs, and members of the pharmaceutical industry. For the current study, we gathered deidentified information from 2020 to 2022 MSK program participants on CD patients’ and HCPs’ attitudes about CD, related to their sense of hope, choice, and loneliness, through anonymous pre-program surveys. Our specific aims were to: (1) Assess differences in perspectives between patients’ and HCPs’ responses in the pre-program survey; (2) Compare patients’ and HCPs’ perceived care goals and unmet needs.
Methods
Educational program enrollment
The MSK program was offered to patients with any type of pituitary tumor as well as HCPs, family members, caregivers, and members of industry. The role of the registrant as a patient, caregiver/family member, HCP, and/or member of industry was determined for all registrants of the virtual programs.
Any patient with a pituitary tumor treated at our center and outside institutions, inclusive of patients at all points along their treatment journey, were invited to register for the virtual education program. HCPs, including endocrinologists, neurosurgeons, otolaryngologists, radiation oncologists, neurologists, ophthalmologists, neuro-oncologists, family medicine and internal medicine physicians, physicians in training and other allied health professionals who treat and manage patients with pituitary diseases were also invited to register. Invitations were sent through email to neuroendocrine experts and endocrinologists, patient support groups on social media, direct messaging to patients with pituitary tumors by their treating physicians and via patient databases, advertisements through endocrine societies, brochure/postcard mailing, and Eventbrite, a virtual platform for live events.
Study participants
Registrants from MSK virtual programs held on December 5, 2020, (n = 328) and April 9, 2022, (n = 327) were included in the pool of subjects, among which the qualifying participants were determined.
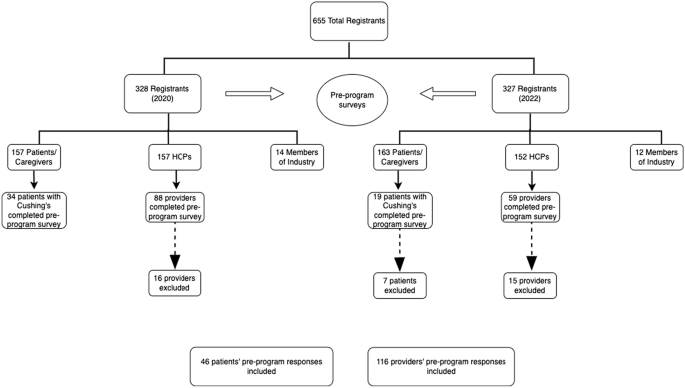
Of the 655 total registrants from the 2020 and 2022 programs, 320 (48.9%) were patients or caregivers and 309 (47.2%) were HCPs (Fig. 1). Of the 147 providers (88 in 2020 and 59 in 2022) that attended and filled out a pre-program survey 31 were excluded from our analysis. Eight filled out surveys in both 2020 and 2022, 4 were members of industry, 3 did not fill out any responses, and 1 was not in the healthcare field. In addition, 12 providers had at least three fields missing in the survey and 3 had filled out two surveys for the same year, so they were also excluded. A total of 116 providers (72 from 2020 to 44 from 2022) were included in the analysis.
Among the 320 pituitary patients who attended the programs (157 from 2020 to 163 from 2022), 53 identified as ‘patients with Cushing’s’ and submitted surveys (34 participants from 2020 to 19 from 2022). Seven patients were excluded from the 2022 surveys as they had also filled out surveys in 2020, leaving a final group of 46 patients who were included in the analysis.
Virtual education programs
For each program, there was a single day of live interactive programming, meaning that all participants attended at the same time. The programs were recorded and made available for several weeks as enduring material for registrants on an online website.
After joint sessions in the morning, both programs consisted of two tracks in the afternoon: the ‘provider/clinical track’ and the ‘patient/caregiver track’. During the programs, an ongoing chat reeled through the virtual program which allowed patients to continually ask questions. Faculty experts answered these questions in written responses directly within the chat and/or in spoken responses during one of the live broadcasted Q&A sessions. Additionally, the programs both included panel discussions answering patient questions and moderated patient discussions with invited patient speakers.
Study procedures
Through anonymous pre-program surveys distributed at the 2020 and 2022 symposia, patients and HCPs answered questions related to their own sense, or perception of their patients’ sense, of hope, choice, and loneliness in the context of living with CD. This survey was developed by a multidisciplinary team and has been reported previously [11]. Demographic and clinical information was also assessed including year of diagnosis, prior treatments, and current medications (for patients) and specialty and practice type (for providers), as shown in Tables 1 and 2. Multiple-choice questions assessing patients’ attitudes toward their disease included possible answers of ‘I have no hope for improvement,’ ‘I have some hope for improvement,’ and ‘I have a lot of hope for improvement;’ and ‘I have no choice in my treatment,’ ‘I have some choices in my treatment,’ and ‘I have many choices in my treatment.’ Patients were also asked to respond ‘TRUE’ or ‘FALSE’ to the following statements: ‘I feel alone living with my Cushing’s,’ ‘Hearing the journeys of other patients helps me better understand my own,’ and ‘I feel anxious about my Cushing’s diagnosis.’
Multiple-choice questions assessing providers’ attitudes about their patients’ Cushing’s included possible answers of ‘I have no hope for their improvement,’ ‘I have some hope for their improvement,’ and ‘I have a lot of hope for their improvement;’ and ‘my patients have no choice in their treatment,’ ‘my patients have some choices in their treatment,’ and ‘my patients have many choices in their treatment.’ Providers were also asked to respond ‘TRUE’ or ‘FALSE’ to the following statements: ‘my patients feel alone living with their Cushing’s,’ ‘Hearing the journeys of other patients helps will help my patients better understand their own,’ and ‘my patients feel anxious about their Cushing’s diagnosis.’
Additionally, patients were surveyed on care goals and unmet needs related to their treatment. Specifically, patients were asked, ‘What are the healthcare outcomes/goals that matter to you the most?’ and ‘What do you think are unmet needs for the diagnosis or treatment of your condition?’ The first question was intended to refer to the patient specifically, while the second question was meant to examine how the condition is treated in general. Survey responses were submitted as free text and subsequently grouped by the authors (AH and EBG) into nine different categories: (a) Quality of life (QoL)/Mental Health; (b) Medical Therapies/Tumor Control; (c) Education/Awareness; (d) Communications/Multidisciplinary Care; (e) Insurance/Access; (f) Fertility; (g) Controlling Comorbidities; (h) Support System and (i) none. Responses could receive multiple designations if applicable. AH coded the free text themes independently, then EBG reviewed each answer and corresponding grouping to confirm accuracy. If there was disagreement or confusion, coding from our prior work [11] was reviewed.
HCPs were also surveyed on care goals and unmet needs related to their patient’s treatment. Providers were asked, ‘What are the healthcare outcomes/goals that matter to you the most?’ and ‘what do you think are unmet needs for the diagnosis or treatment of your patient’s condition?’ The first question was intended to refer to the provider and their goals related to Cushing’s, while the second question was meant to examine how the condition is treated in general. Survey responses were submitted as free text and subsequently grouped by the authors (AH and EBG) into nine different categories: (a) Quality of life (QoL)/Mental Health; (b) Medical Therapies/Tumor Control; (c) Education/Awareness; (d) Communications/Multidisciplinary Care; (e) Insurance/Access; (f) Fertility; (g) Controlling Comorbidities; (h) Support System and (i) none. Responses could receive multiple designations if applicable.
Statistical analysis
Descriptive statistics were presented as counts and percentages for categorical variables and as medians and interquartile range (IQR) for continuous variables. The Chi-square test or Fisher’s exact test was used to compare gender and survey responses between the CD patient group and the HCP group. All statistical tests were two-tailed, and a P-value of < 0.05 was considered statistically significant. SAS Software® (version 9.4; SAS Institute Inc., Cary, NC) was used for all analyses.
Results
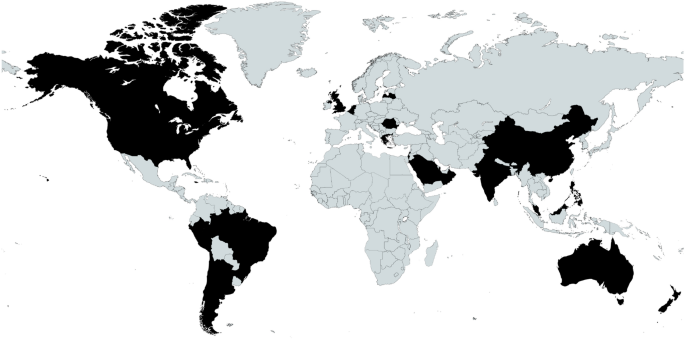
Between the 2020 and 2022 events, there was combined representation from 25 different countries. A map and a full list of the countries is shown in Fig. 2.
Fig. 2
Map of registrant locations. Locations (listed alphabetically): Argentina, Australia, Belgium, Brazil, Canada, Chile, China, Greece, Hong Kong, India, Israel, Jamaica, Latvia, Malaysia, Netherlands, New, Zealand, Oman, Peru, Philippines, Qatar, Romania, Saudi Arabia, Singapore, UK, US
From a total of 655 participants over two educational events, 46 patients with CD and 116 HCP caring for CD patients were included in the analysis. The demographic data of the patients and HCPs are outlined in Tables 1 and 2, respectively. Median age of the patients and HCPs was 51 years. 78.3% of the CD group was female vs. 53.0% of the HCP group (P = 0.003).
CD patients ranged from newly diagnosed to being diagnosed 33 years prior. The HCPs who filled out the pre-program surveys were in practice for a mean duration of 18.5 years, with a range from 1 to 54 years.
As shown in Table 1, CD patients had a mean duration of suspected active disease prior to diagnosis of 5.26 years, as defined by onset of CD symptoms until diagnosis, and a mean duration of disease since diagnosis of 5.9 years. 42 (91%) had undergone surgical treatment of their Cushing’s. For those who underwent surgery, the mean number of surgeries was 1.17 (range 0–4). 20% had received pituitary radiation. Overall, 31% of patients were on medical therapy for Cushing’s. Metyrapone was the most used CD therapy (in 11%), followed by ketoconazole (in 9%). Of those requiring pituitary hormone replacement, 34.8% had one pituitary hormone deficiency and 21.7% had multiple hormone deficiencies. Thyroid hormone replacement (37%) and adrenal replacement (30%) were the most common.
As shown in Table 2, the majority of the HCPs were endocrinologists (72%) followed by neurosurgeons (9%) and nurses (8%). There was a total of 9 different specialties represented by the provider group. 16% of the providers worked in private practice, 16% were hospital based, and 16% worked in ‘unspecified clinical care.’ 38% of the providers practice type was ‘unspecified.’
Based on the pre-program survey responses, we identified different attitudes between patients and HCPs in several domains. Table 3 depicts pre-program survey responses from CD patients and HCPs assessing their attitudes about CD. 21.7% of patients reported they had no choices in their treatment, compared to 0.9% of HCPs (P < 0.001). Almost all HCPs (99.1%) reported that CD patients had least some choice in their management. In addition, less than half (45.7%) of patients reported they had a lot of hope for improvement whereas 71.3% of HCPs had a lot of hope for their patients’ improvement. Surprisingly, fewer CD patients reported feeling anxious about their diagnosis compared to HCPs’ perceived patient anxiety (65.2% vs 94.6%, P < 0.001). However, more patients tended to feel more alone living with CD than HCPs’ perception of such (60.9% vs. 45.5%, P = 0.08). Both CD patients and HCPs agreed that hearing the journeys of other CD patients would help patients better understand their own disease (97.8% vs 100%).
Table 3 Patient and provider attitudes by pre-program survey
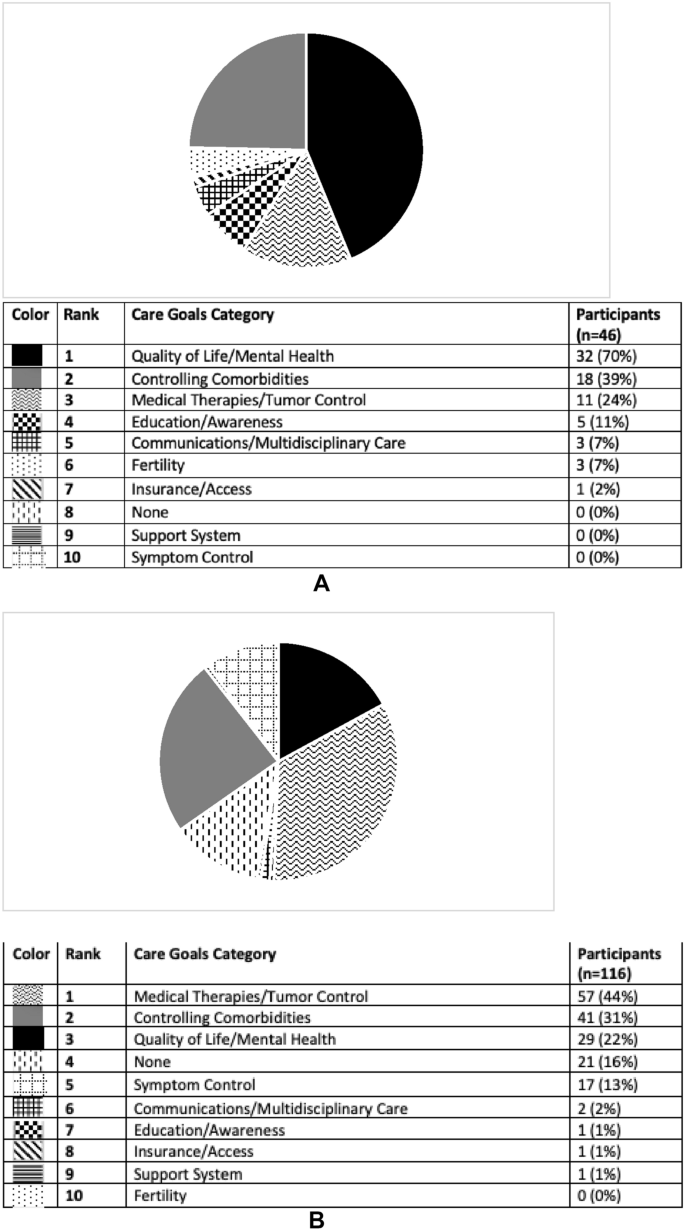
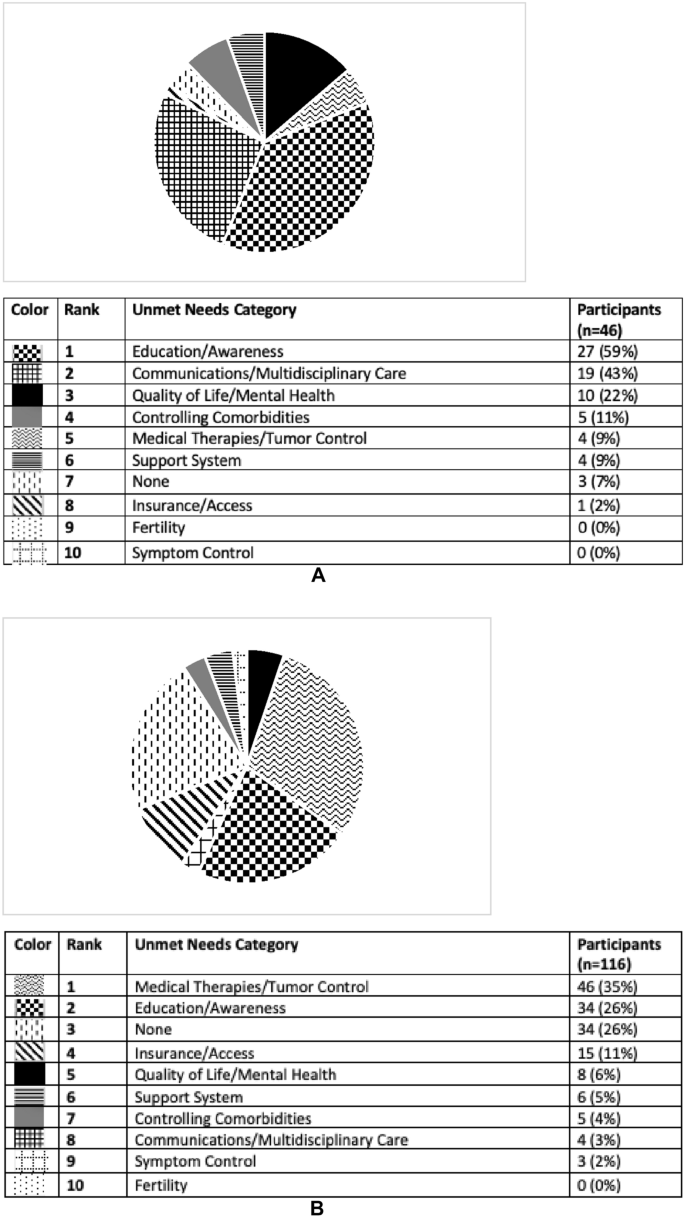
CD patients and HCPs were also surveyed on their personal care goals and unmet needs, results of which are shown in Figs. 3A, B and 4A, B. The most common personal care goal concern for patients was ‘QoL/mental health’ which was reported by 70%, followed by ‘controlling comorbidities’ (39%) and ‘medical therapies/tumor control’ (24%). HCPs prioritized the same three care goals as patients but ‘medical therapies/tumor control’ was the most common (44%). ‘Controlling comorbidities’ and ‘QoL/mental health’ were the second and third most often HCP reported care goals (31 and 22% respectively). ‘Education/awareness’ was the most common perceived CD unmet need by patients (59%). HCPs reported both ‘medical therapies/tumor control’ and ‘education/awareness’ to be the most common unmet needs (35 and 26%, respectively). Examples of patient and provider responses, and how they were coded, are shown in Supplemental Table 1.
Fig. 3
A Care goals according to participants with Cushing’s who completed pre-program survey. This pie graph represents the free-text survey response from patients regarding their personal care goals as categorized by topic. B Care goals according to providers who completed pre-program survey. This pie graph represents the free-text survey response from providers regarding their personal care goals as categorized by topic
A Unmet needs for the field of Cushing’s disease according to participants with Cushing’s who completed pre-program survey. This pie graph represents the free-text survey response from patients regarding unmet needs in Cushing’s as categorized by topic. B Unmet needs for the field of Cushing’s disease according to providers who completed pre-program survey. This pie graph represents the free-text survey response from providers regarding unmet needs in Cushing’s as categorized by topic
This study examined the differences between patients and HCP-reported perceptions of living with CD. We identified several differences in disease outlook between CD patients and HCPs. We found that more patients than HCPs reported they had no choices in their treatment. Furthermore, less than half of patients reported they had a lot of hope for improvement whereas most (71.3%) of HCPs had a lot of hope for their patients’ improvement. Interestingly, fewer CD patients reported feeling anxious about their diagnosis compared to HCPs’ perceived patient anxiety, although a higher percentage of patients reported feeling alone living with CD compared to the HCPs’ perception of patient loneliness. We also identified HCP and patient differences in reported personal care goals and perceived unmet needs in the field. The most common personal care goal concern for patients was ‘QoL/mental health,’ whereas it was ‘medical therapies/tumor control’ for HCPs. ‘Education/awareness’ was the most commonly perceived unmet need by patients, whereas it was ‘medical therapies/tumor control’ for HCPs.
Our findings support prior work demonstrating a discrepancy between patients and HCPs regarding the need for improved multidisciplinary care [12]. 43% of patients listed ‘communication/multidisciplinary care’ as an unmet need in the field, compared to 3% of providers. Pituitary centers of excellence provide expert multidisciplinary care in the neuroendocrine, neurosurgical, and radiation oncology domains, but often lack expertise in mental and physical health domains salient for CD patients, who suffer from depression, anxiety, myopathy and joint pain. In order to offer comprehensive care, psychiatrists, psychologists, social workers, pain medicine experts, physical therapists, and nutritionists with expertise in CD should be included in the pituitary center multidisciplinary team [13]. Our findings suggest that pituitary centers of excellence should take into account the most important personal care goal reported by CD patients, which is Qol/mental health, and provide expert treatment in this domain.
It is not surprising that Qol/mental health is the personal care goal most reported by CD patients. Prior assessment of acromegaly patients demonstrated the same finding: QoL/mental health was the most common personal care goal concern [11]. While surgical [14] and medical [15,16,17,18] treatment of Cushing’s improves QoL, QoL has been shown to remain impaired over time after treatment [19]. Several factors may contribute to long-term Qol impairments, including the presence of persistent disease, imperfect treatment modalities which themselves may be associated with burden and adverse side effects, and persistent comorbidities including depression, anxiety, fatigue, and overweight. Perception of disease status may also play a role in QoL. In surgically remitted CD patients, there may be discordance between biochemical remission and perceived disease status [8]. Specifically, this study found that of those with self-identified persistence of disease, 65% were in fact biochemically remitted. This group had lower QoL scores than the concordant group who self-identified as in remission with biochemical evidence of remission.
CD patients’ outlook on their condition, including their perception of choices and hope for change, has not been previously well described, despite the fact that these perceptions likely inform long term Qol. Patient outlook may be a modifiable target that if addressed, could improve long term patient well-being and outcomes. Aside from continuing progress in the development of new therapies for CD patients which can offer patients more objective choices in their treatment, other modalities should be considered. Prior work has shown that virtual educational programs improve acromegaly patients’ hope for improvement, perception of having choices in their treatment, and sense of loneliness [11]. Educational programs have also been shown to result in improved physical activity and sleep, and reduced pain levels in CS patients [20]. More work is needed to develop effective education programming tailored for CD patients to provide the appropriate support that these patients need.
Difference in HCP and patient disease perceptions may also play a role in Cushing’s patients’ quality of life and outcomes. Among a cohort of patients who underwent surgical resection for Cushing’s, 32.4% reported not receiving information from their doctors about the recovery experience, despite the fact that all physicians surveyed reported giving information about the recovery process [9]. Furthermore, 16.1% of patients in this cohort reported that not enough medical professionals were familiar with the symptoms of Cushing’s. Recovery time was also reported to be longer by patients than providers [9]. Similarly, discordance was found between acromegaly patients and HCPs regarding reported severity of symptoms, with patients more frequently reporting symptoms as severe compared to HCPs, and many patients reporting symptoms which were not reported by HCPs [6]. Improving communication between HCP and patients may positively affect CD patient outlook and QoL.
We identified a similar disparity between CD patients and HCP regarding care goals and unmet needs. 70% of patients surveyed considered QoL/mental health to be a top care goal, but only 22% of provider shared this goal. 59% of patients reported education/awareness as an unmet need, compared to 26% of HCPs. These findings support data shown by Acre et al. in which Cushing’s patients report a lack of symptom recognition by their providers [9]. HCPs should be aware that their patients may have different treatment priorities.
Our finding that more HCPs reported patient anxiety living with CD compared to patients themselves needs further exploration. This could reflect inadequate communication between HCP and patient, or skewed HCP perceptions of CD. This, and other findings in our study should be viewed in light of the small cohort, and as such, needs confirmation in larger cohorts and more in-depth symptom assessments. Additional limitations of our study include lack of paired patient-HCP responses as the HCPs included were not providing care for this specific CD cohort. Since this was a pituitary educational forum, likely most or all patients who identified as having Cushing’s had CD. However, our survey did not specify the type of surgery patients underwent or the etiology of their Cushing’s. Additionally, we used multidisciplinary team agreed upon measures and not validated assessments. Further work should consider validating a tool to assess patient-provider discordances. Our findings may also be confounded by selection bias, given that the patients participating in our virtual education programs are more likely to be under the care of experts in the field and may not represent the attitudes of all patients living with CD. Finally, the included HCPs were representatives from a range of specialties with different levels of experience taking care of patients with CD which may also affect their responses.
Our findings highlight the importance of understanding CD patients’ outlook and perspective in their condition, and that they may differ from their HCP. More than half of CD patients did not have a lot of hope for improvement and reported feeling alone, and many patients felt they had no choices in their treatment. QOL/mental health was the most commonly reported care goal for patients, which was not the case for HCPs. Comprehensive multidisciplinary care for CD patients should include mental health professionals with expertise in CD. Regular open communication between HCPs and CD patients will help bridge perception differences and facilitate personalized care, which will ultimately improve long-term outcomes for CD patients.
Data availability
The data that support the findings of this study are available from the authors upon request.
Kreitschmann-Andermahr I, Siegel S, Gammel C et al (2018) Support needs of patients with Cushing’s disease and Cushing’s syndrome: results of a survey conducted in Germany and the USA. Int J Endocrinol 2018:9014768. https://doi.org/10.1155/2018/9014768
Feelders RA, Pulgar SJ, Kempel A, Pereira AM (2012) The burden of Cushing’s disease: clinical and health-related quality of life aspects. Eur J Endocrinol 167(3):311–326. https://doi.org/10.1530/EJE-11-1095
Donegan D, Gowan T, Gruber R et al (2021) The need for patient-centered education among patients newly diagnosed with a pituitary tumor. J Endocr Soc. https://doi.org/10.1210/jendso/bvab061
Geer EB, Sisco J, Adelman DT et al (2020) Observed discordance between outcomes reported by acromegaly patients and their treating endocrinology medical provider. Pituitary 23(2):140–148. https://doi.org/10.1007/s11102-019-01013-2
Carluccio A, Sundaram NK, Chablani S et al (2015) Predictors of quality of life in 102 patients with treated Cushing’s disease. Clin Endocrinol (Oxf) 82(3):404–411. https://doi.org/10.1111/cen.12521
Acree R, Miller CM, Abel BS, Neary NM, Campbell K, Nieman LK (2021) Patient and provider perspectives on postsurgical recovery of Cushing syndrome. J Endocr Soc. https://doi.org/10.1210/jendso/bvab109
Ca BM, Badiu C, Bonomi M et al (2017) Developing and evaluating rare disease educational materials co-created by expert clinicians and patients: the paradigm of congenital hypogonadotropic hypogonadism. Orphanet J Rare Dis 12(1):57. https://doi.org/10.1186/s13023-017-0608-2
Valassi E, Santos A, Yaneva M et al (2011) The European registry on Cushing’s syndrome: 2-year experience. Baseline demographic and clinical characteristics. Eur J Endocrinol 165(3):383–392. https://doi.org/10.1530/EJE-11-0272
Casanueva FF, Barkan AL, Buchfelder M et al (2017) Criteria for the definition of pituitary tumor centers of excellence (PTCOE): a pituitary society statement. Pituitary 20(5):489–498. https://doi.org/10.1007/s11102-017-0838-2
Santos A, Resmini E, Martinez-Momblan MA et al (2012) Psychometric performance of the Cushing QoL questionnaire in conditions of real clinical practice. Eur J Endocrinol 167(3):337–342. https://doi.org/10.1530/EJE-12-0325
Colao A, Petersenn S, Newell-Price J et al (2012) A 12-month phase 3 study of pasireotide in Cushing’s disease. N Engl J Med 366(10):914–924. https://doi.org/10.1056/NEJMoa1105743
Fleseriu M, Biller BM, Findling JW et al (2012) Mifepristone, a glucocorticoid receptor antagonist, produces clinical and metabolic benefits in patients with Cushing’s syndrome. J Clin Endocrinol Metab 97(6):2039–2049. https://doi.org/10.1210/jc.2011-3350
Geer EB, Salvatori R, Elenkova A et al (2021) Levoketoconazole improves clinical signs and symptoms and patient-reported outcomes in patients with Cushing’s syndrome. Pituitary 24(1):104–115. https://doi.org/10.1007/s11102-020-01103-6
Pivonello R, Fleseriu M, Newell-Price J et al (2020) Efficacy and safety of osilodrostat in patients with Cushing’s disease (LINC 3): a multicentre phase III study with a double-blind, randomised withdrawal phase. Lancet Diabetes Endocrinol 8(9):748–761. https://doi.org/10.1016/S2213-8587(20)30240-0
Page-Wilson G, Oak B, Silber A et al (2023) Evaluating the burden of endogenous Cushing’s syndrome using a web-based questionnaire and validated patient-reported outcome measures. Pituitary. https://doi.org/10.1007/s11102-023-01314-7
Martínez-Momblán MA, Gómez C, Santos A et al (2016) A specific nursing educational program in patients with Cushing’s syndrome. Endocrine 53:199–209. https://doi.org/10.1007/s12020-015-0737-0
The authors would like to thank the HCP and patient participants who attended the events, the MSK faculty, invited speakers, Leslie Edwin of Cushing’s Support and Research Foundation, Amy Edouard and the MSK CME team, and Recordati Rare Diseases, Inc., Amryt Pharma (previously Chiasma, Inc.), Crinetics, Sparrow Pharmaceuticals, Corcept Therapeutics, and Xeris Biopharma (previously Strongbridge Biopharma) for providing educational grants for these educational activities.
Funding
This research was funded in part through the NIH/NCI Cancer Center Support Grant P30 CA008748.
Author information
Authors and Affiliations
Division of Endocrinology, Department of Medicine, Weill Cornell Medicine, New York, NY, USA
Amanda Halstrom
Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, NY, USA
I.-Hsin Lin
Multidisciplinary Pituitary & Skull Base Tumor Center, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Andrew Lin, Marc Cohen, Viviane Tabar & Eliza B. Geer
Department of Neurology, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Andrew Lin
Department of Neurosurgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Andrew Lin, Marc Cohen & Eliza B. Geer
Head and Neck Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Marc Cohen & Viviane Tabar
Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Eliza B. Geer
Contributions
A.H. and E.B.G. wrote the manuscript text and prepared the figures. All authors reviewed the manuscript.
As an educational quality initiative project using de-identified data, it was determined that our project did not constitute human subjects research and thus did not require IRB oversight.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The following is a summary of “Treatment of Cushing Disease With Pituitary-Targeting Seliciclib,” published in the March 2023 issue of Endocrinology & Metabolism by Liu, et al.
Seliciclib (R-roscovitine) has been shown in preclinical studies to inhibit neoplastic corticotroph proliferation and the production of adrenocorticotropic hormone (ACTH) in the pituitary gland. Therefore, for a study, researchers sought to investigate the effectiveness of seliciclib as a pituitary-targeting treatment for patients with Cushing’s disease (CD).
Two prospective, open-label, phase 2 trials were conducted at a tertiary referral pituitary center. Adult patients with de novo, persistent, or recurrent CD received oral seliciclib 400 mg twice daily for four consecutive days each week for four weeks. The primary endpoint in the single-center study was normalization of 24-hour urinary free cortisol (UFC; ≤ 50 µg/24 hours) at the end of the study, and in the multicenter study, the primary endpoint was UFC normalization or a ≥ 50% reduction in UFC from baseline to the end of the study.
Of the 16 patients who consented, 9 were treated with seliciclib. The mean UFC decreased by 42% from 226.4 ± 140.3 µg/24 hours at baseline to 131.3 ± 114.3 µg/24 hours at the end of the study. The longitudinal model showed significant reductions in UFC from baseline to each treatment week. Three patients achieved a ≥ 50% reduction in UFC (range, 55%-75%), and two exhibited a 48% reduction; none achieved UFC normalization. Plasma ACTH decreased by 19% (P = 0.01) in patients with ≥48% UFC reduction. Three patients developed grade ≤ 2 elevated liver enzymes, anemia, and/or elevated creatinine, resolved with dose interruption/reduction. Two patients developed grade 4 liver-related serious adverse events that resolved within four weeks of seliciclib discontinuation.
The results suggested that seliciclib may target pituitary corticotrophs in CD and reverse hypercortisolism. Although potential liver toxicity of seliciclib resolves with treatment withdrawal, a further determination is required to establish the lowest effective dose.
Importance Pituitary adenomas may hypersecrete hormones or cause mass effects. Therefore, early diagnosis and treatment are important.
Observations Prevalence of pituitary adenomas ranges from 1 in 865 adults to 1 in 2688 adults. Approximately 50% are microadenomas (<10 mm); the remainder are macroadenomas (≥10 mm).
Mass effects cause headache, hypopituitarism, and visual field defects. Treatments include transsphenoidal surgery, medical therapies, and radiotherapy. Prolactinomas account for 32% to 66% of adenomas and present with amenorrhea, loss of libido, galactorrhea, and infertility in women and loss of libido, erectile dysfunction, and infertility in men; they are generally treated with the dopamine agonists cabergoline and bromocriptine.
Growth hormone–secreting tumors account for 8% to 16% of tumors and usually present with enlargement of the lips, tongue, nose, hands, and feet and are diagnosed by elevated insulin-like growth factor 1 levels and growth hormone levels; initial treatment is surgical. Medical therapy with somatostatin analogues, cabergoline, and pegvisomant is often also needed.
Adrenocorticotropic hormone (ACTH)–secreting tumors account for 2% to 6% of adenomas and are associated with obesity, hypertension, diabetes, and other morbidity. Measurement of a late-night salivary cortisol level is the best screening test but petrosal sinus sampling for ACTH may be necessary to distinguish a pituitary from an ectopic source.
The primary treatment of Cushing disease (hypercortisolism due to ACTH-producing adenomas, which is the cause in approximately 65% of the cases of hypercortisolism) is adenoma resection and medical therapies including ketoconazole, mifepristone, and pasireotide.
Hyperthyroidism due to thyroid-stimulating hormone–secreting tumors accounts for 1% of tumors and is treated with surgery and somatostatin analogues if not surgically cured. Clinically nonfunctioning adenomas account for 15% to 54% of adenomas and present with mass effects; surgery is generally required, although incidentally found tumors can be followed if they are asymptomatic.
Conclusions and Relevance Patients with pituitary adenomas should be identified at an early stage so that effective treatment can be implemented. For prolactinomas, initial therapy is generally dopamine agonists. For all other pituitary adenomas, initial therapy is generally transsphenoidal surgery with medical therapy being reserved for those not cured by surgery.
RSS Error: A feed could not be found at `http://www.oconnormusic.org/feed.xml`; the status code is `503` and content-type is `text/html; charset=us-ascii`
RSS Error: A feed could not be found at `http://www.oconnormusic.org/bios.xml`; the status code is `503` and content-type is `text/html; charset=us-ascii`