..The doctor’s first thought was that Elvis had had a seizure and he injected him with a stimulant to improve his breathing. Then he and Elvis’s manager dragged him into the ensuite bathroom and managed to get him into the bath, which they filled with cold water. Soon they were dressing him in his stage clothes.
Incredibly Elvis managed to perform that night, leaving Dr Nick determined to find out what had caused the handsome man he first met to degenerate into the bloated figure he had become.
Elvis himself refused to give him any clues. Finally, one of his problems was revealed – he and Priscilla were getting divorced. Three days after the final decree was issued in California, the singer, in worse condition than he had ever been, chartered a plane back to Graceland and called for Dr Nick.
This time the doctor arrived to find his patient’s face puffy, pink and almost transparent, and his stomach distended. He suspected either an allergic reaction or heart failure, especially since heart disease ran in the family.
Hospital tests established that Elvis had hepatitis, an enlarged liver ( possibly from painkillers) and Cushing’s syndrome. The last was a hormonal disease that caused bloating, and was down to the many steroids he had been taking to combat the asthma that ran in the family and his ongoing colon problems.
When Dr Nick asked him why he was also covered in bruises, Elvis tried to tell him the marks were from acupuncture needles. Finally he confessed that a couple of Beverly Hills physicians had prescribed the narcotic Demerol to cure back and neck pain, and Novocaine to reduce the pain at the injection sites…
After 8 years of menopause-like symptoms, a 62 year old patient discovered she actually had Cushing’s disease. Read about her long journey to get a diagnosis and her success in finding her dream-come-true neurosurgeon.
A Mysterious Decline in Health
When Elisabeth N., 62, started developing symptoms that included obesity, osteoporosis, insomnia, kidney stones and hair loss, she attributed it to what most women her age would: menopause. Back in 2000 she never would have thought those seemingly normal symptoms for a woman her age would lead her to Santa Monica to be treated eight years later by Daniel Kelly, MD., neurosurgeon and director of the Pacific Pituitary Disorders Centerat Pacific Neuroscience Institute and Saint John’s Health Center. In fact, it wasn’t till February of 2008 that she learned it could all be caused by something completely different.
A Sister’s Observation Leads to a Breakthrough
“I wouldn’t have known about Cushing’s disease if it weren’t for my youngest sister; I’m 25 years older and so fortunate she has her medical degree,” explained Elisabeth, a kitchen and bath designer in Mesa, Arizona. “We hadn’t seen one another for five years when we visited in February of 2008. My appearance had drastically changed by then. She told me, ‘Don’t be scared, Bethie, but I think you should be tested for Cushing’s.’”
Learning About Cushing’s Disease
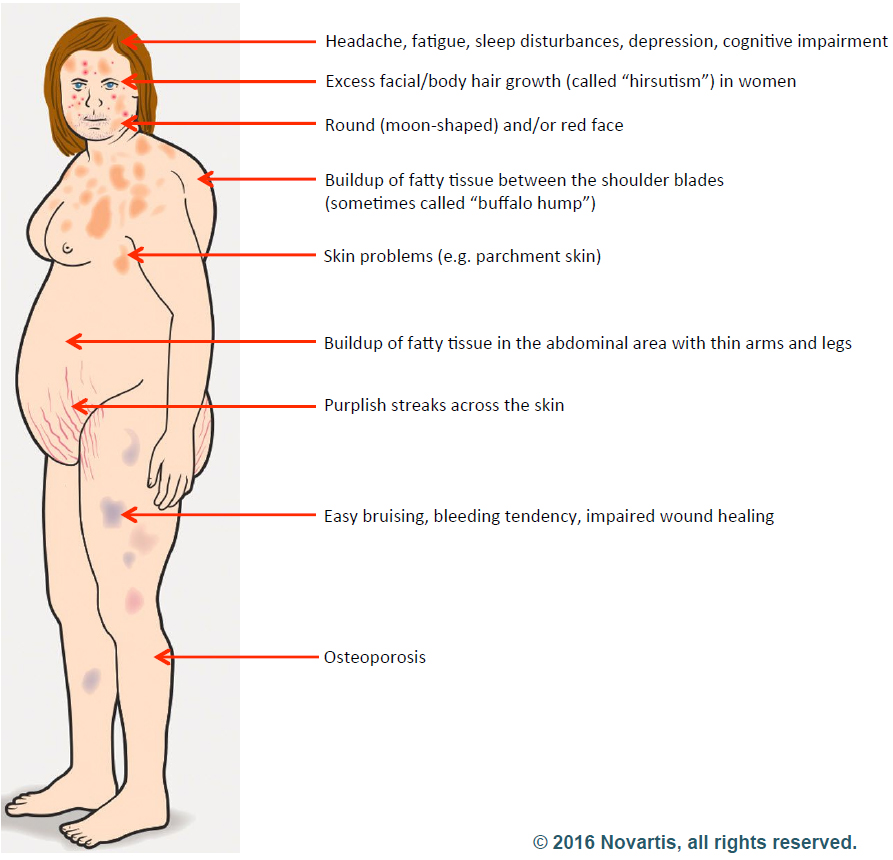
Elisabeth started researchingCushing’s disease right away and was relieved to learn that a cure was possible. Cushing’s is a hormonal disorder caused by high levels of the hormone cortisol. Symptoms include upper-body obesity, fragile skin that bruises easily, weakened bones, severe fatigue, weak muscles, high blood pressure, high blood glucose, increased thirst and urination, depression and a fatty hump between the shoulders. Women can also experience irregular menstrual periods and excess hair growth on their bodies. It can be caused by taking glucocorticoids such as prednisone or if there is a problem with a person’s pituitary gland or hypothalamus.
A Long and Uncertain Testing Journey
Elisabeth immediately set up a doctor’s appointment to get her cortisol and adrenocorticotropic hormone (ACTH – the pituitary hormone that stimulates the adrenal glands to make cortisol) levels tested. Over the next nine months Elisabeth went through several blood, urine, saliva and plasma tests for her cortisol and ACTH production and had an MRI. The tests showed elevated cortisol and ACTH levels but the initial impression was that her levels were not high enough to indicate Cushing’s disease and her pituitary MRI showed no apparent tumor. Elisabeth met with both a pituitary neurosurgeon and an endocrinologist, but both determined her condition not to be Cushing’s.
“My cortisol was not high enough; I wasn’t obese enough; I wasn’t disabled enough; I wasn’t depressed enough,” Elisabeth said.
Finding the Missing Clue
She felt frustrated by the diagnosis and continued to research possibilities online. It was during this research that she stumbled upon an article comparing MRI Tesla strengths. It recommended getting a Tesla 3.0 with contrast to pick up small abnormalities. Elisabeth scheduled a new MRI at the beginning of November. This time the scan detected a 6 mm tumor on the right side of her pituitary gland. Additional hormonal testing also confirmed that she did indeed have high ACTH and cortisol levels consistent with Cushing’s, “I was thrilled to finally have proof I had Cushing’s, but terrified because I knew I’d have to have brain surgery to remove it,” Elisabeth said. “I knew I wanted transsphenoidal surgery – the safest, most successful procedure with the least complications if done by an experienced surgeon.”
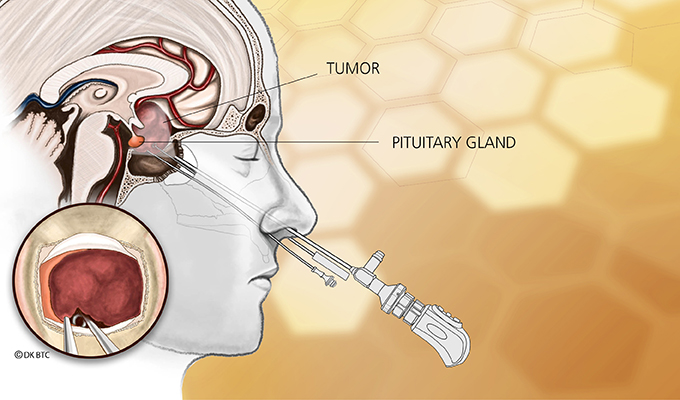
Understanding the Endonasal Transsphenoidal Approach
Endonasal transsphenoidal tumor removal, aka endoscopic endonasal approach, such as what Elisabeth needed, is a surgery that uses the nostril as the entry point with visualization from the operating microscope and endoscope. The approach passes through the back of the nasal cavity and into the sphenoid sinus to the skull base without facial incisions, brain retraction or post-operative nasal packing.
“This type of surgery is ideal for removing over 99% of pituitary adenomas, like what Elisabeth had and is considered first-line therapy for patients with Cushing’s disease,” Dr. Kelly explained. “Untreated or incompletely treated, Cushing’s disease is a very serious condition leading to uncontrolled hypertension, diabetes, weight gain and increased mortality.”
Choosing the Right Surgeon
With all the months she had to prepare for a diagnosis, Elisabeth knew exactly what needed to be done.
“I’d known I wanted Dr. Kelly to perform surgery but never imagined it could happen,” Elisabeth said. “I found him online. He’s ranked as one of the world’s top neurosurgeons specializing in this type of surgery. While watching his YouTube videos, I was awed by his kindness, patience, sense of humor, approachability, professionalism and complete lack of arrogance in spite of his fame. I’m still pinching myself that I had the fortune and honor to become one of his patients.”
A Life-Changing Call
Figuring she didn’t have anything to lose, Elisabeth called Dr. Kelly’s office and asked if he was accepting new patients (he was) and how long was his waiting list (she could see him next week). Elisabeth was astounded. She immediately mailed Dr. Kelly all the test results, films and reports she could gather.
“Two days later, Dr. Kelly personally called and left a message, indicating it appeared there was indeed an ACTH secreting adenoma on my pituitary gland and to call him back,” Elisabeth said. “I was blown away. I’d have expected to win the lottery first.”
Successful Surgery and a New Beginning
Dr. Kelly arranged to perform Elisabeth’s surgery two weeks later on November 26 – the day before Thanksgiving. Her cortisol levels fell dramatically within 24 hours of surgery. She has remained in remission since then. Years after surgery, she continues to feel like a new person and regularly stays in contact with Dr. Kelly and his office staff.
About Dr. Daniel Kelly
Dr. Daniel Kelly, a board-certified neurosurgeon, is the director and one of the founders of the Pacific Neuroscience Institute, director of the Pacific Brain Tumor Center and Pacific Pituitary Disorders Center, and is Professor of Neurosurgery at Saint John’s Cancer Institute at Providence Saint John’s Health Center. Considered to be one of the top neurosurgeons in the US, he is a multiple recipient of the Patients’ Choice Award and Southern California Super Doctors distinction.
Obesity is common at diagnosis of pituitary adenoma in childhood and may persist despite successful treatment, according to findings published in Clinical Endocrinology.
“The importance of childhood and adolescent obesity on noncommunicable disease in adult life is well recognized, and in this new cohort of patients, we report that obesity is common at presentation of pituitary adenoma in childhood and that successful treatment is not necessarily associated with weight loss,” Aashish Sethi, MD, MBBS, a pediatric endocrinologist in the department of endocrinology at Alder Hey Children’s Hospital in Liverpool, United Kingdom, and colleagues wrote. “We have reported obesity, and obesity-related morbidity in a mixed cohort of children and young adults previously, but [to] our knowledge, this is the first time this observation has been reported in a purely pediatric cohort.”
In a retrospective study, Sethi and colleagues analyzed clinical and radiological data from 24 white children from Alder Hey Children’s Hospital followed for a median of 3.3 years between 2000 and 2019 (17 girls; mean age at diagnosis, 15 years). Researchers assessed treatment modality (medical, surgical or radiation therapy), pituitary hormone deficiencies and BMI, as well as results of any genetic testing.
Within the cohort, 13 girls had prolactinomas (mean age, 15 years), including 10 macroadenomas between 11 mm and 35 mm in size. Children presented with menstrual disorders (91%), headache (46%), galactorrhea (46%) and obesity (38%). Nine children were treated with cabergoline alone, three also required surgery, and two were treated with the dopamine agonist cabergoline, surgery and radiotherapy.
Five children had Cushing’s disease (mean age, 14 years; two girls), including one macroadenoma. Those with Cushing’s disease presented with obesity (100%), short stature (60%) and headache (40%). Transsphenoidal resection resulted in biochemical cure; however, two patients experienced relapse 3 and 6 years after surgery, respectively, requiring radiotherapy. One patient also required bilateral adrenalectomy.
Six children had a nonfunctioning pituitary adenoma (mean age, 16 years; two girls), including two macroadenomas. These children presented with obesity (67%), visual field defects (50%) and headache (50%). Four required surgical resections, with two experiencing disease recurrence after surgery and requiring radiotherapy.
During the most recent follow-up exam, 13 children (54.1%) had obesity, including 11 who had obesity at diagnosis.
“The persistence of obesity following successful treatment, in patients with normal pituitary function, suggests that mechanisms other than pituitary hormone excess or deficiency may be important,” the researchers wrote. “It further signifies that obesity should be a part of active management in cases of pituitary adenoma from diagnosis.” – by Regina Schaffer
Disclosures: The authors report no relevant financial disclosures.
When we become stressed out bodies release cortisol – the stress hormone – which helps us cope with challenges. Cortisol’s role is to convert protein into energy by releasing glycogen and counteract inflammation. When cortisol is released in the body temporarily, this is okay and won’t have long-lasting detrimental effects to health as it is a natural response to a stressor. But when cortisol levels remain high chronically it can eventually begin to tear your body down thus causing health complications. This is why numerous health experts recommend the reduction of stress as much as possible because in the long run it can harm our health.
High cortisol levels over the long term can destroy healthy muscle and bone, slow down healing, impair digestion, metabolism and mental function, and weaken the immune system. Additionally, adrenal fatigue has been linked to numerous other health conditions including fibromyalgia, hypothyroidism, chronic fatigue syndrome, arthritis, premature menopause, and many others. High cortisol levels are also associated with many unwanted symptoms which we will outline below.
High cortisol symptoms
If you’re concerned about your cortisol levels, the following signs and symptoms associated with high cortisol levels can alert you and prompt you to make the necessary changes in order to reduce cortisol levels.
Unexplained weight gain
Skin symptoms including acne, skin infections, lesions, thin-appearing skin, bruising, growing facial hair, and reddish purple streaks on skin
Muscle and bone symptoms like a deep pain in the bones, weak muscles, chronic backaches, increased risk of bone fractures
Gender specific changes such as women developing male-pattern hair growth, irregular menstrual cycles, low libido, infertility
Neurological symptoms such as depression, irritability, headaches, chronic fatigue, and anxiety
High blood pressure (hypertension)
Poor sleep or lack of sleep
Swelling of hands and feet
If you notice any of the above symptoms, you may want to have your cortisol levels checked to confirm diagnosis. Living with high cortisol levels over the long term can have detrimental effects on a person’s health. Treating high cortisol as soon as possible can lower the risk of long-term health problems.
Causes of high cortisol
There are two main causes of high cortisol: Chronic stress and more rarely, Cushing’s disease. Cushing’s disease is caused by a hormone-secreting tumor on the adrenal gland which results in the release more cortisol than required.
Living with chronic stress also leads to high cortisol because the release of cortisol is a natural response from the body when it is stressed. The hypothalamic–pituitary-adrenal [HPA] axis is what regulates the timely release of cortisol during acute stress, but when stress becomes chronic the feedback from the HPA becomes damaged and so cortisol continues to be released.
Conditions that can contribute to chronic stress and high cortisol include:
Depression
Panic disorder
Generalized anxiety disorder
Post traumatic stress disorder (PTSD)
Anorexia nervosa
Bulimia nervosa
Alcoholism
Diabetes
Severe obesity
Metabolic syndrome
Polycystic ovary syndrome (PCOS)
Obstructive sleep apnea
Working in shifts
End-stage kidney disease
Chronic pain
Tips to lower high cortisol
Here are some tips that can help you lower your high cortisol levels and thus prevent long-term health problems associated with high cortisol. [MaryO’Note:These will not work if you have active Cushing’s! You must remove the source of your Cushing’s first.]
Eat a well balanced meal with plenty of fruits and vegetables, avoid sugars, consume low glycemic index foods, avoid processed foods, eat a wide variety of health foods to ensure you receive all essential vitamins and nutrients
Exercise on a regular basis
Take time out of each day to relax – listen to music, meditate, pray, perform your favorite hobby, anything that promotes relaxation
Take up yoga or tai chi
Ensure you are getting adequate sleep
Drink tea
Watch funny videos or hang out with a funny friend
Go for a massage
Do something spiritual – attend a service
Chew gum
Limit caffeine intake
Stretch
By incorporating these helpful tips into your life you will find that your high cortisol symptoms begin to diminish and your overall health begins to improve.
I think that this is so important, especially with our health. Had I not been an active participant and followed several doctors’ advice 25 years ago, I’d most likely not been here to write this.
I see this all the time, though. Whatever the doctor says is true. People will say that the doctor gave me this or that med but they don’t know what it is for.
I just don’t get how people can take meds and not have a clue what they are, how they work, how they might interact with other drugs they may be taking. But it happens because people blindly follow whatever a doctor may give them.
Participation is so important – you have to know how YOU’RE feeling, what YOUR symptom are. Do your own research. Your doctor doesn’t know what it feels like to live in your body no matter how much you try to tell him/her.
Ultimately, you are the one who cares most about yourself and the only one who can make a difference through your research, thoughts and actions.
Just because a doctor gives you something, you don’t have to take it. 24 years ago a locally well-known neurologist “gave me” Xanax. Since he couldn’t see my tumor with his Magnetic Resonance Imaging (MRI) machine there was “no possibility” that it existed. Had I followed his advice, taken the Xanax and stopped pursuing a Cushing’s diagnosis I would most have likely died by now.
The doctor was going by the odds. The odds were that I really didn’t have a pituitary tumor. But I’m not a statistic and neither are you. Follow your instincts and take care of YOU. This is the only life you’ll ever have.
The most healing thing we can do for ourselves is to participate in the process of our lives as fully as we can-even when the unexpected and the fearful happen.
~Today’s Page-a-Day calendar
What do YOU do to keep participating in your health care and daily life?