LAS VEGAS — Higher doses of mifepristone for Cushing’s disease (Korlym) weren’t associated with increases in serious adverse events, researchers reported here.
Korlym is a glucocorticoid receptor antagonist better known as RU-486, or the “abortion pill.” It was approved for treating hyperglycemia associated with Cushing’s disease in 2012.
In an analysis of data from the SEISMIC trial, Dat Nguyen, MD, and colleagues found that similar percentages of patients had serious adverse events across all doses of the drug, reported.
They also reported at the American Association of Clinical Endocrinologists meeting here, that the proportion of the four most common adverse events — headache, fatigue, nausea, and hypokalemia — fell off after 10 weeks of the 24-week trial.
“Recent prescription data indicate that many physicians are not titrating beyond 300 mg per day, potentially limiting patients’ clinical response,” the researchers said.
The 2012 approval was based on the SEISMIC study, which followed 50 Cushing’s disease patients over 24-weeks in an open-label format. It found that daily doses improved blood sugar control and reduced insulin requirements.
Clinicians participating in the trial were told they could titrate beyond the starting dose of 300 mg a day. To look at the relationship between dose and safety, as well as response, Nguyen and colleagues looked at data on 40 of the patients who responded to therapy.
Most of them (90%) were taking at least 600 mg a day, 68% were taking at least 900 mg per day, and 44% took 1,200 mg daily.
Most of the responders (85%) had their initial clinical response at a dose of at least 600 mg daily.
Overall, there were 26 serious adverse events:
- 10 at the 300 mg dose
- 8 at the 600 mg dose
- 3 at the 900 mg dose
- 3 at the 1200 mg dose
- 2 while off drug
When the researchers adjusted for the number of patients who had ever reached a given dose, the frequency of serious adverse events was similar across doses:
- 10% of patients at 300 mg
- 16% of patients at 600 mg
- 15% of patients at 900 mg
- 14% of patients at 1200 mg
The four most common adverse events decreased after week 10 – although that tracked an increase in dose (mean 588 mg/day before week 10 versus 895 mg/day thereafter).
Nguyen and colleagues concluded that higher doses of mifepristone weren’t associated with increases in serious adverse events or in the most common adverse events – and that better response was seen with higher doses.
Korlym was developed by Corcept Therapeutics of Menlo Park, Calif., as an orphan drug given that it is is believed only 5,000 patients are eligible for treatment. That gave the company 7 years of exclusive rights to market the agent for Cushing’s disease.
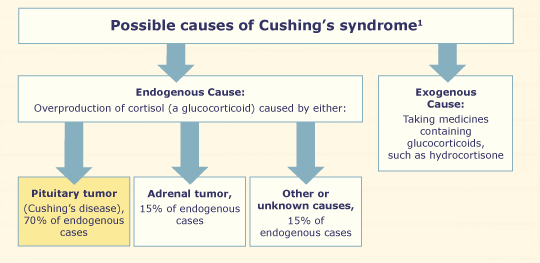
The label limits the drug’s indication to patients with endogenous Cushing’s disease who have type 2 diabetes or glucose intolerance and aren’t candidates for surgery, or failed to respond to surgical intervention.
The drug doesn’t reduce cortisol production but prevents it from binding to its receptor – an action separate from its blockade of the progesterone receptor, which makes it an effective agent in abortion.
Since the daily doses are in the same range as those used to induce abortion, the drug is contraindicated in pregnant women. It also carries a boxed warning that the drug will terminate a pregnancy.
Filed under: Cushing's, pituitary | Tagged: blood sugar, cortisol, Cushing's Disease, fatigue, headache, hyperglycemia, hypokalemia, Insulin, Korlym. RU-486, mausea, mifepristone, SEISMIC | Leave a comment »