Cushing’s disease patients who exhibit nodules or masses in their lungs should be thoroughly investigated to exclude fungal infection with Cryptococcus neoformans, a study from China suggests.
While rare, the infection can be life-threatening, showing a particularly worse prognosis in patients with fluid infiltration in their lungs or with low white blood cell counts in their blood.
The study, “Cushing’s disease with pulmonary Cryptococcus neoformans infection in a single center in Beijing, China: A retrospective study and literature review,” was published in the Journal of the Formosan Medical Association.
Cortisol, a hormone that is produced in excess in Cushing’s disease patients, is a kind of glucocorticoid that suppresses inflammation and immunity. Consequently, subjects exposed to cortisol for long periods, much like immuno-compromised patients, are at high risk for infections.
In Cushing’s patients, the most common infections include Pneumocystis jiroveci, Aspergillus fumigatus, and Cryptococcosis — 95 percent of which are caused by C. neoformans.
But while “Cushing’s disease patients are susceptible to C. neoformans, the association between pulmonary C.neoformans and [Cushing’s disease] is poorly explored,” researchers said.
In an attempt to understand the clinical characteristics of Cushing’s patients who develop C.neoformans infections, researchers in Beijing, China, reviewed the clinical records of six patients at their clinical center.
Their analysis also included six other patients whose cases had been reported in previous publications.
Patients had a mean age of 44 and 10 were diagnosed initially with high blood pressure. Seven also had diabetes mellitus.
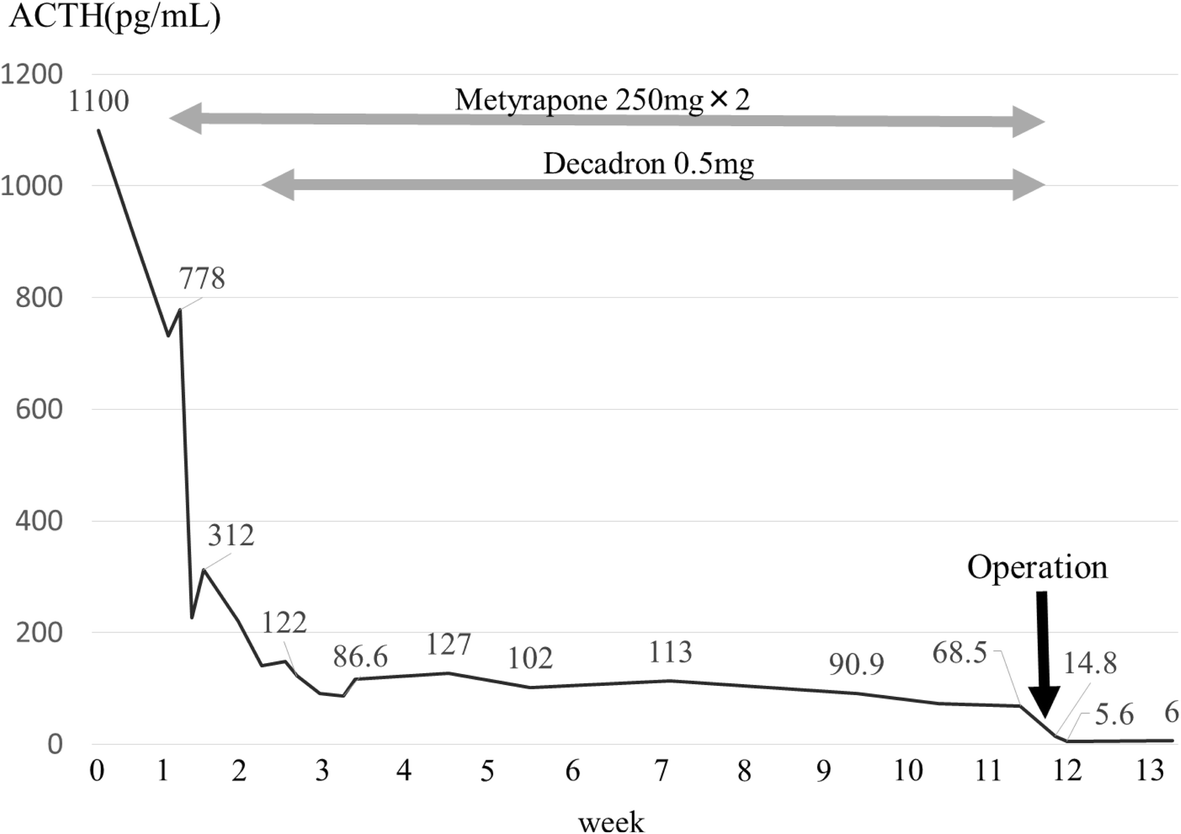
All patients had elevated cortisol levels in their urine and high levels of the adrenocorticotropic hormone (ACTH). Ultimately, all patients were found to have masses in their pituitary glands, causing the high cortisol and ACTH levels.
Patients complained of lung symptoms, including shortness of breath after physical activity, cough, and expectoration. But they had no fever or signs of blood in the lungs, which could suggest lung infection.
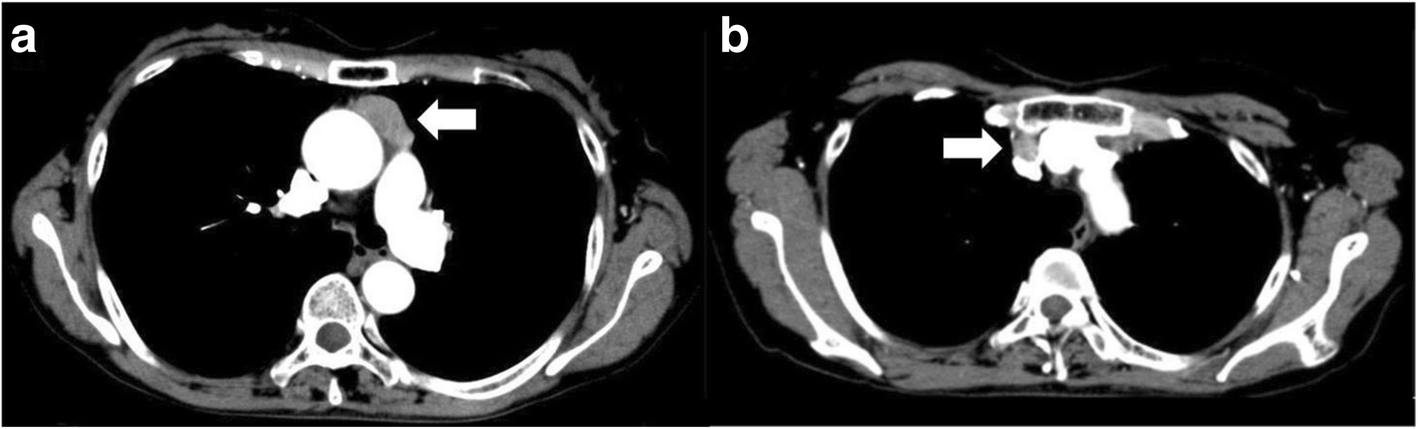
A CT scan of the chest then revealed lung nodules in four patients, and lung masses in five patients. Four patients, including one with a lung mass, also had lung air spaces filled with some material (pulmonary consolidation), which was consistent with pulmonary infection.
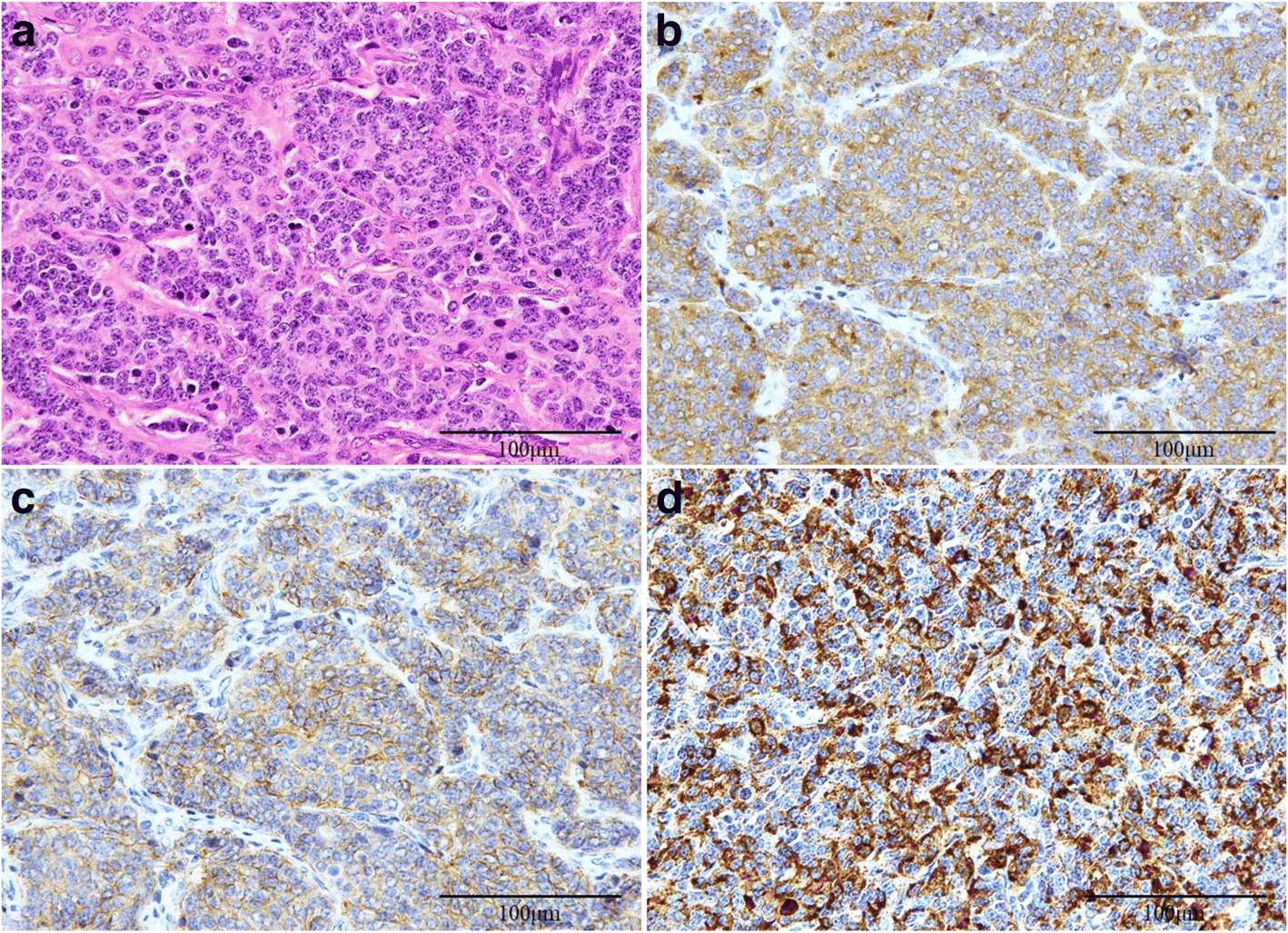
After analyzing lung nodule/mass biopsies, lung fluids, or blood samples, all patients were diagnosed with C. neoformans pulmonary cryptococcosis.
For their infection, patients received anti-fungal drugs, including amphotericin-B, fluconazole, flucytosine, and liposomal amphotericin. Cushing’s disease, however, was treated with surgery in 10 patients and ketoconazole in two patients.
Despite the treatments, five patients died during follow-up, including four who experienced co-infections or spreading of the cryptococcal infection and one patient with extensive bleeding after surgical removal of the gallbladder.
Among them, two patients had significantly low white blood cell levels and elevated cortisol levels, and four had infiltration in their lungs, suggesting these are markers of poor prognoses.
Researchers also noted that the patients who received ketoconazole died during in the reviewed studies. They attribute this to ketoconazole’s anti-fungal properties, which may interfere with its ability to manage Cushing’s symptoms.
Given the high susceptibility of Cushing’s disease patients to C. neoformans infections, “pulmonary nodules or masses should be aggressively investigated to exclude” this potentially fatal opportunistic infection, the researchers suggested.
“The infiltration lesions in chest CT scan and lymphopenia seem to be potential to reflect the poor prognosis,” they said.
Filed under: Cushing's, pituitary, Rare Diseases | Tagged: ACTH, blood pressure, Cryptococcus neoformans, Cushing's Disease, diabetes, infection, lung, nodules, pituitary | Leave a comment »