


A Cushing’s diagnosis can be a long and frustrating event with testing, repeat testing, redoing testing.
Sometimes, I think that this was the path that some of my UFCs took on the way to my diagnosis:
It took three years from 1983 to 1986 before doctors would consider testing me for Cushing’s, even though I was sure that this was what my problem was.
My first 24-hour urine free cortisol was run by a Hematologist/Oncologist. After that, things seemed to move a little better, if not faster. That UFC got me to my first endo.
The Endocrinologist, of course, didn’t trust the other test so I was back to square one. He ran his own multitude of tests. He had to draw blood at certain times like 9 AM. and 5 PM. There was a dexamethasone suppression test where I took a pill at 10 p.m. and gave blood at 9 am the next day.
 I collected gallons of urine in BIG boxes (Fun in the fridge!). Those were from 6 a.m. to 6 a.m. to be delivered to his office by 9 a.m. same day. I was always worried that I’d be stopped in rush hour and the police would ask about what was in that big container. I did those daily for a week.
I collected gallons of urine in BIG boxes (Fun in the fridge!). Those were from 6 a.m. to 6 a.m. to be delivered to his office by 9 a.m. same day. I was always worried that I’d be stopped in rush hour and the police would ask about what was in that big container. I did those daily for a week.
When the endo confirmed that I had Cushing’s in 1987 he sent me to a local hospital where they repeated all those same tests for another week and decided that it was not my adrenal gland (Cushing’s Syndrome) creating the problem. The doctors and nurses had no idea what to do with me, so they put me on the brain cancer ward.
When I left this hospital after a week, we didn’t know any more than we had before.
As luck would have it, NIH (National Institutes of Health, Bethesda, Maryland) was doing a clinical trial of Cushing’s. I live in the same area as NIH so it was not too inconvenient but very scary at first to think of being tested there. At that time I only had a choice of NIH, Mayo Clinic and a place in Quebec to do this then-rare pituitary surgery called a Transsphenoidal Resection. I chose NIH – closest and free. After I was interviewed by the Doctors there, I got a letter that I had been accepted into the clinical trial. The first time I was there was for 6 weeks as an inpatient. More of the same tests.
Six weeks of daily UFC testing. To this day, I still remember nurses waking me just after 6 am to “close out your urine”. Sounded like a bank account!
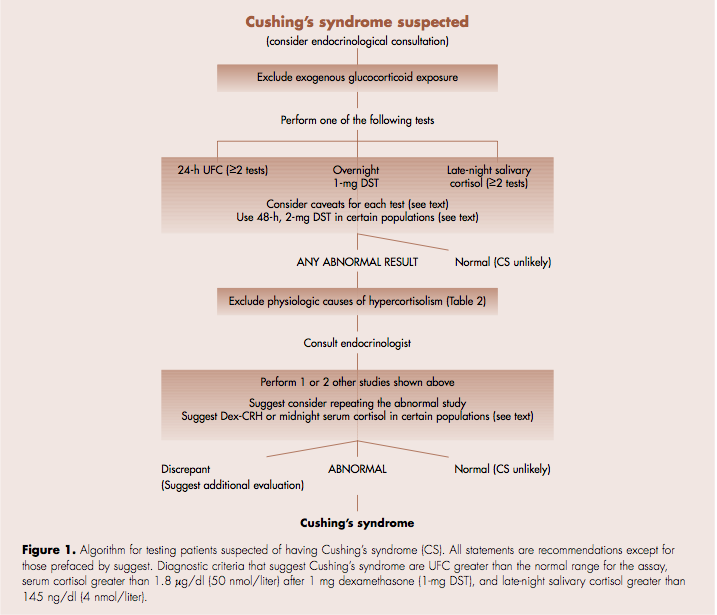
The testing pathway today looks a little more organized but it still takes far too long:
Filed under: Clinical trials, Cushing's | Tagged: 24-hour urine free cortisol test, blood tests, clinical trial, dexamethasone suppression test, endocrinologist, Hematologist/Oncologist, National Institutes of Health, NIH, pituitary, transsphenoidal, UFC | Leave a comment »


