Integration of Clinical Studies With Case Presentations
Maria Fleseriu, Richard J Auchus, Irina Bancos, Beverly MK Biller Journal of the Endocrine Society, Volume 9, Issue 4, April 2025, bvaf027 https://doi.org/10.1210/jendso/bvaf027
Abstract
Although most cases of endogenous Cushing syndrome are caused by a pituitary adenoma (Cushing disease), approximately one-third of patients present with ectopic or adrenal causes.
Surgery is the first-line treatment for most patients with Cushing syndrome; however, medical therapy is an important management option for those who are not eligible for, refuse, or do not respond to surgery.
Clinical experience demonstrating that osilodrostat, an oral 11β-hydroxylase inhibitor, is effective and well tolerated comes predominantly from phase III trials in patients with Cushing disease. Nonetheless, reports of its use in patients with ectopic or adrenal Cushing syndrome are increasing. These data highlight the importance of selecting the most appropriate starting dose and titration frequency while monitoring for adverse events, including those related to hypocortisolism and prolongation of the QT interval, to optimize treatment outcomes. Here we use illustrative case studies to discuss practical considerations for the management of patients with ectopic or adrenal Cushing syndrome and review published data on the use of osilodrostat in these patients.
The case studies show that to achieve the goal of reducing cortisol levels in all etiologies of Cushing syndrome, management should be individualized according to each patient’s disease severity, comorbidities, performance status, and response to treatment. This approach to osilodrostat treatment maximizes the benefits of effective cortisol control, leads to improvements in comorbid conditions, and may ameliorate quality of life for patients across all types and severities of Cushing syndrome.
Ectopic adrenocorticotropic hormone secretion (EAS) is responsible for approximately 10%–18% of Cushing’s syndrome cases. Thymic neuroendocrine tumors (NETs) comprise 5%–16% of EAS; therefore, they are very rare and the data about this particular tumors is scarce.
We present a case of a 34-year-old woman with a rapid onset of severe hypercortisolism in April 2016. After initial treatment with a steroid inhibitor (ketoconazole) and diagnostics including 68Ga DOTA-TATE PET/CT, it was shown to be caused by a small thymic NET.
After a successful surgery and the resolution of all symptoms, there was a recurrence after 5 years of observation caused by a metastasis to the breast, shown in the 68Ga DOTA-TATE PET/CT result and confirmed with a breast biopsy.
Treatment with a steroid inhibitor (metyrapone) and tumor resection were again curative. The last disease relapse appeared 7 years after the initial treatment, with severe hypercortisolism treated with osilodrostat. There was a local recurrence in the mediastinum, and a thoracoscopic surgery was performed with good clinical and biochemical effect.
The patient remains under careful follow-up. Our case stays in accordance with recent literature data, showing that patients with thymic NETs are younger than previously considered and that the severity of hypercortisolism does not correlate with the tumor size. The symptoms of EAS associated with thymic NET may develop rapidly and may be severe as in our case. Nuclear medicine improves the effectiveness of the tumor search, which is crucial in successful EAS therapy. Our case also underlines the need for lifelong monitoring of patients with thymic NETs and EAS.
1 Introduction
Ectopic adrenocorticotropic hormone secretion (EAS) represents between 9% and 18% of adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome (CS) cases (1–3). The tumors secreting ACTH may occur in many locations and present with different histopathological differentiation, resulting in various clinical outcomes. In the past, most of the EAS cases were associated with small cell lung cancer, characterized by rapid tumor progression and unfavorable prognosis. Recently, well-differentiated neuroendocrine tumors (NETs) from the foregut prevail in the clinical series of EAS, with most common locations in the lungs, thymus, and pancreas (1).
EAS is often associated with severe hypercortisolism. Typical Cushing’s appearance may not be present due to the rapid onset of the disease. Patients with this type of hypercortisolism need urgent treatment because they have the highest mortality of all forms of CS (4). A retrospective review of 43 patients with EAS reported deaths in 27 patients (62.8%) and a median overall survival of 32.2 months. The leading causes of mortality were the progression of primary malignancies and systemic infections; two patients died from pulmonary embolism (5).
Prompt surgical removal of the tumor secreting ACTH is the mainstay of the therapy. However, finding the tumor causing EAS can be challenging due to its small size and variety of locations. Most authors recommend a combination of computed tomography (CT) scanning of the chest, abdomen, and pelvis, with additional magnetic resonance imaging (MRI) of the pituitary, as the first-line examinations (1, 6, 7). However, the sensitivity of standard imaging modalities is suboptimal (8). In the analysis of 231 patients with EAS, cross-sectional imaging revealed the source of ACTH in 52.4% of them at initial evaluation, and another 29% was found during follow-up or due to nuclear medicine functional imaging, while 18.6% remained occult (9). Nuclear medicine improves the sensitivity of conventional radiology in the case of EAS, with the use of 18-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET)/CT (18F-FDG PET/CT) expected to be useful in identifying EAS tumors with high proliferative activity and 68gallium-labeled somatostatin analogues (68Ga DOTA-TATE) PET/CT with the potential to detect NETs. In the head-to-head comparison, the detection rate of the source of EAS was 75% for 68Ga DOTA-TATE and 60% for 18F-FDG PET/CT, while the highest sensitivity (90%) was achieved when both methods were combined (10).
Thymic NETs comprise 2%–5% of all thymic neoplasms and may cause some paraneoplastic syndromes, with the most frequent being myasthenia gravis, syndrome of inappropriate antidiuretic hormone secretion, and hypercortisolism (11). EAS associated with thymic NETs are rare, representing between 5% and 16% of EAS in published case series (1). Because of the rarity and heterogeneity of the disease, no evidence-based guidelines are available.
We present a case of a patient with thymic NET causing EAS, with metastasis to the breast after 5 years of post-surgical remission and another local recurrence 7 years after the first operation.
Our case is unique because thymic NETs causing EAS are known as an aggressive disease with a median recurrence time of 24 months after thymectomy (12). There are only a few cases described of metastases to the breast from thymic NETs causing EAS (13–16). Moreover, 68Ga-SSTR PET/CT was very helpful in detecting both primary and metastatic ectopic ACTH-secreting tumor, which underlines its role in the diagnostic workout of EAS.
2 Case description
A 32-year-old woman with no relevant medical history was admitted to the endocrinology department in April 2016 due to the rapid onset of symptoms: weight gain, hypertension, skin changes, and oligomenorrhoea.
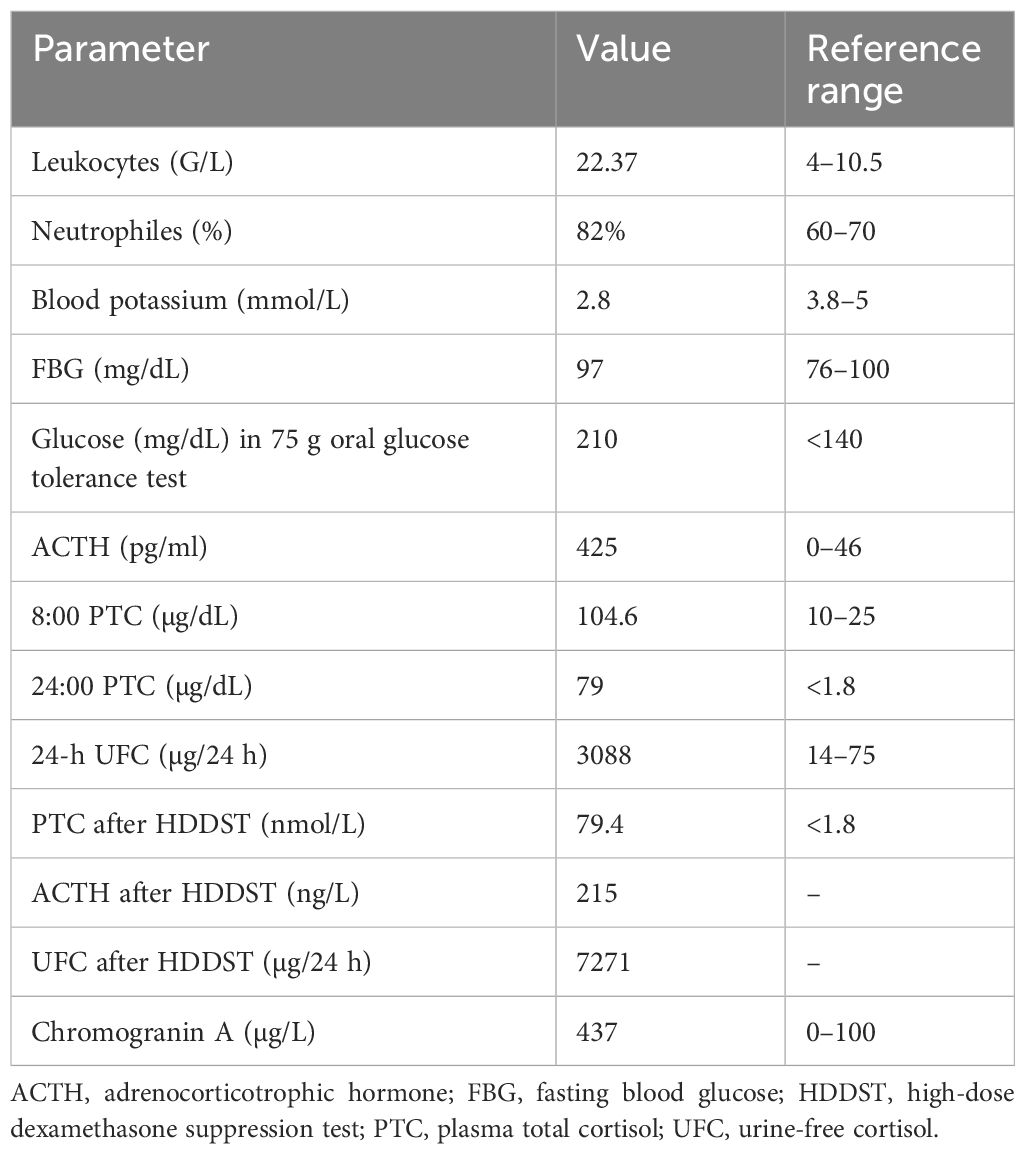
The measurements at initial physical examination were as follows: body mass index (BMI)—29 kg/m2, blood pressure—180/90 mmHg, and heart rate—88/min. She had plethora, acne, moon face, buffalo hump, central obesity, many red striae in the abdominal area, and mild hirsutism. The baseline laboratory findings are presented in Table 1, with hypokalemia, diabetes, leukocytosis, high levels of serum cortisol, ACTH, and chromogranin A, and increased urine-free cortisol (UFC) secretion. There was no suppression of serum cortisol or UFC after a high-dose dexamethasone test. ACTH-dependent CS was diagnosed, and EAS was suspected. The patient’s family history was negative for endocrine diseases or genetic disorders.
Table 1
Table 1. Laboratory results at diagnosis (April 2016).
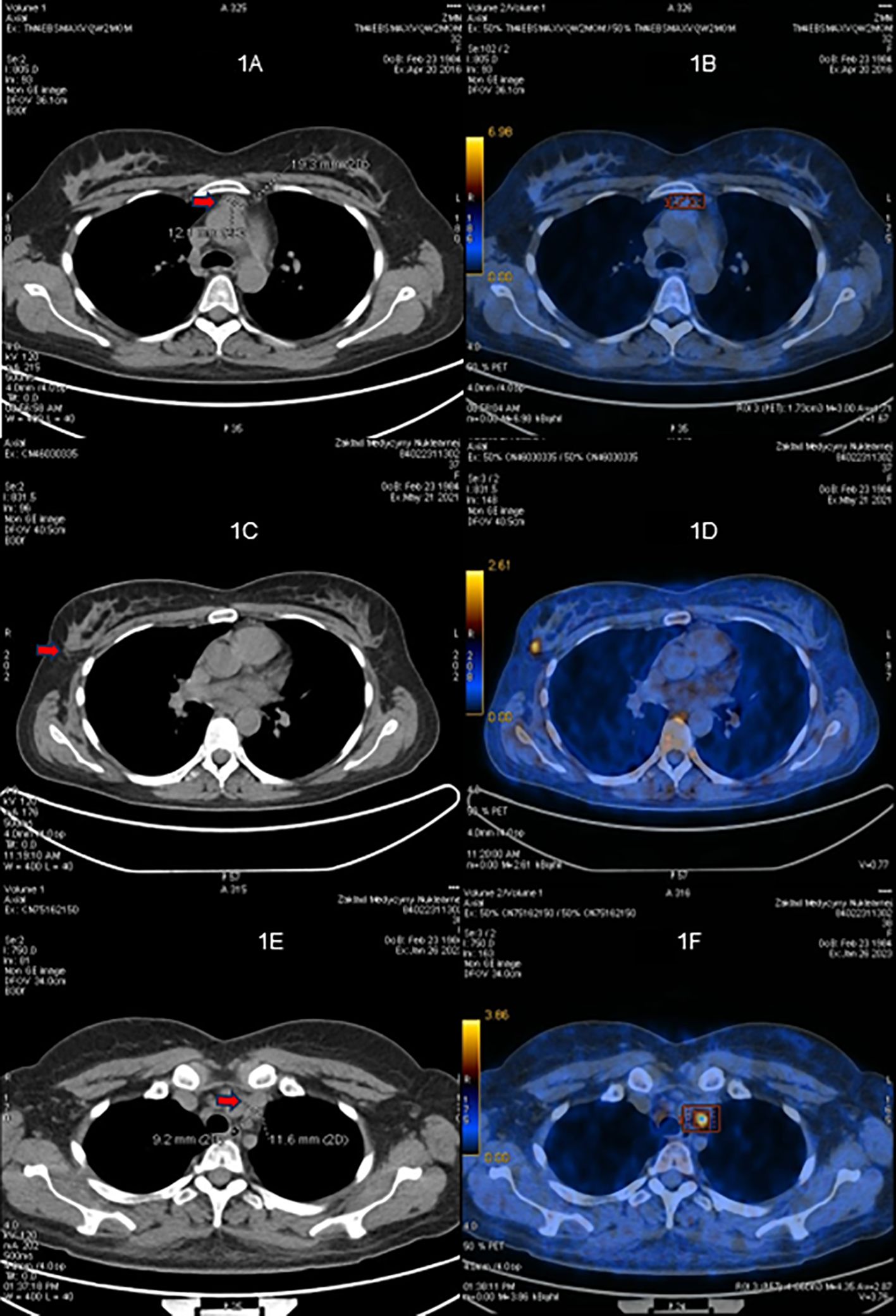
The first-line cross-sectional imaging studies (chest, abdomen, and pelvis CT and MRI of the pituitary gland) did not reveal the source of ACTH. Only a symmetrical enlargement of adrenals was observed. 68Ga DOTA-TATE PET/CT revealed an oval lesion in the anterior mediastinum (1.9 × 1.3 cm) with a subtle overexpression of somatostatin receptors (SUV max. 2.8, Figures 1A, B). The chest MRI confirmed a mass 1.5 × 2.0 × 2.5 cm, with high T2-weighted signal and high contrast enhancement, suggestive of NET. The patient was given ketoconazole (600 mg daily), spironolactone, potassium supplementation, antihypertensive drugs, and thromboembolic prophylaxis. In June 2016, thoracoscopic removal of the mediastinal tumor was performed. In the histopathological examination, the tumor was encapsulated, without evidence of invasion, and no lymph node metastases were described. The immunophenotype of the tumor was as follows: CgA (+), Syn (+), CKAE1+E3 (+) “dot-like”, S100 (-), calcitonin (-), EMA (+/-), Ki67 3% to 4% in hot spots, no necrosis, mitotic index 0/10HPF with conclusion: thymic NET—typical carcinoid (low-grade). The presence of paraganglioma was also taken into consideration, as such cases were described (17). However, the significant reaction with cytokeratin and lack of S100 protein expression made this diagnosis less probable.
Figure 1
Figure 1. 68Ga-DOTATATE PET/CT scans. (A, B) Before the first surgery (April 2016). (C, D) Before the second surgery (May 2021). (E, F) Before the third surgery (January 2023).
The postoperative morning serum cortisol concentration was below 5 µg/dL, indicating biochemical remission. The patient received hydrocortisone substitution for a month. The clinical signs of CS disappeared, and there was a normalization of UFC.
During 5 years of follow-up, the patient got pregnant and delivered a healthy child. Genetic counseling was performed, and no germline mutation of MEN1 gene was identified. Other clinical manifestations of MEN1 (like primary hyperparathyroidism and pituitary secreting tumors) were excluded.
In May 2021, the patient experienced a sudden recurrence of CS symptoms. The laboratory findings confirmed severe hypercortisolism (Table 2); therefore, treatment with steroid inhibitor metyrapone was administered. The patient tolerated only 750 mg daily; there were side effects (skin rash and tachycardia) with higher doses. The chest MRI revealed no recurrence in the location of the primary tumor, only a lesion in the right breast (1.2 × 1.0 × 1.1 cm) with atypical contrast enhancement. The 68Ga-DOTA-TATE PET/CT result showed a subtle overexpression of the tracer (SUV max 1.9) in the right breast (Figures 1C, D). Breast ultrasonography confirmed a hypoechogenic, hypervascular mass in the right breast, BIRADS 3/4, diagnosed as NET in the breast biopsy. The tumor was removed in July 2021 without complications. The histopathological samples were compared with the primary lesion, confirming the metastasis from thymic NET to the breast—tumor size 0.7 × 1.5 cm, clear surgical margins (8 mm) with Ki67 3% (NET G2), and no lymph node metastases. After the breast surgery, the cortisol levels normalized in blood and urine and the CS symptoms disappeared. 18F-FDG PET/CT and 68Ga-DOTA-TATE PET/CT were performed, showing no pathological increase of radiotracer uptake in post-operative locations or mediastinal lymph nodes. The patient consulted with the oncology team, and no adjuvant therapy was recommended.
Table 2
Table 2. Laboratory results during 7 years of observation.
The next recurrence of the disease occurred in February 2023, with the symptoms developing suddenly during a very short period (1 to 2 weeks), additionally with significant mental deterioration (concentration disorders, anxiety, severe mood swing). The laboratory findings confirmed excessive hypercortisolism (Table 2). The patient was given osilodrostat (the initial dose was 20 mg daily but later reduced to 10 mg daily for 2 weeks until surgery) and symptomatic treatment with good clinical and biochemical effect. The 68Ga-DOTA-TATE PET/CT result showed a slightly increased uptake of the tracer in the left mediastinum, between cervical vessels, 0.9 × 1.2 cm (Figures 1E, F)—probably a local recurrence. Thoracotomy was performed in February 2023, with subsequent clinical and biochemical improvement (Table 2). In the histopathological examination, mediastinal NET G1 was diagnosed, without necrosis, mitotic activity 0/2 mm2, immunophenotype CgA (+), CD56 (+), Ki 67 1%, CK AE1/AE3 (+), CD117 (+), p40 (-), TdT (-), PAX8 (-), and the presence of tumor cell embolism in the vessels. One metastatic lesion was found in the pericardium (the maximal dimension of the tissue was 13 mm, resected radically). Two metastatic lesions in the fat tissue were found (one tissue fragment from the mediastinum, max. 16 mm diameter, and the second tissue fragment was surrounding the jugular vein, max. diameter up to 40 mm, both resected radically). Two of the 10 resected lymph nodes had metastatic lesions: one from the area of the jugular vein, diameter 11 mm, with capsular invasion, and the second lymph node N2R with capsular invasion, both resected radically. The symptoms of hypercortisolism disappeared, and the cortisol values were normalized after the operation. The patient is currently under careful monitoring, without signs of clinical or biochemical recurrence. 68Ga-DOTA-TATE PET/CT is performed every 6 months.
3 Discussion
Our case is representative for thymic NETs causing EAS presented in literature, but it also shows some distinct features, giving new insight into this rare condition.
In recent series, ACTH-secreting thymic NETs occurred often in young adults, like our patient. The typical age of presentation is 21–35 years in the largest case series, and 7.4% were children under 15 years (12, 13). In contrast, the former series of thymic NETs showed a peak incidence in the sixth decade of life (11).
ACTH-secreting thymic NETs show a slight male preponderance (58.6%); however, the patient’s gender does not seem to relate with the disease outcome (12). There was only an association between male sex and larger tumor size preoperatively as found in one case series (13).
Thymic NETs causing EAS are very rarely associated with MEN1; we have also excluded it in our patient. On the contrary, 30% of thymic NETs not associated with CS are found in patients with MEN1, mostly male smokers (18). It is not clear why thymic NETs with EAS are less likely caused by MEN1 gene mutation, but the possibility of this genetic predisposition should always be taken into consideration.
Thymic NETs associated with EAS are generally considered aggressive, presenting significant cellular atypia in the histopathological examination (19). However, the biology of the tumors is variable. In the histopathological examination of 92 thymic NETs secreting ACTH, the most common subtype was atypical NET (46.7%), while 30.4% of the cases were typical NETs and 21.7% were carcinomas, with the median Ki-67 10%, ranging from 1% to 40%. The median tumor size among 112 patients was 4.7 cm, ranging from 1 to 20 cm, and 55.7% of patients had metastases at presentation (12). It proves the significant heterogeneity of the disease.
Our patient had typical NET with small dimensions and localized disease at the time of diagnosis. Despite this, we observed aggressive Cushing’s syndrome with a short duration of symptoms and life-threatening hypokalemia. It has been observed that there is no correlation between tumor size and hormone levels (12). Thymic NETs associated with EAS are often large, which simplifies the diagnosis and localization. However, in the case of incidental sellar mass or small thymic tumor, the differential diagnosis might be difficult. The highest sensitivity in distinguishing thymic EAS from Cushing’s disease was documented in inferior petrosal sinus sampling and corticotropin-releasing hormone (CRH) stimulation test (12, 20).
In severe cases, when small ACTH-secreting NET needs to be found urgently, PET/CT is a very helpful diagnostic tool. In a prospective study comprising 20 patients with histologically proven EAS, the 68Ga-DOTATATE PET/CT result correctly identified the tumor in 75%, with SUV max. ranging from 1.4 to 20.7, while the 18F-FDG PET/CT findings had a slightly worse result (identified 60% tumors), with SUV max. ranging from 1.8 to 10.0. Those methods are believed to be complementary in case of localization and discrimination of EAS. The 68Ga-DOTATATE PET/CT result revealed tumor in six cases with a negative 18F-FDG PET/CT result, while the 18F-FDG PET/CT procedure was diagnostic in three cases with a negative 68Ga-DOTATATE uptake; the combined sensitivity of both methods was 90% (10). The typical first-line diagnostic modalities’ (CT and MRI) sensitivities range from 52% to 66% (9). Our case remains in accordance with those results, showing difficulties in localizing the ACTH source in first-line radiological methods and with 68Ga-DOTATATE PET/CT being the most useful diagnostic tool. It should also be noted that the 68Ga-DOTATATE uptake was only mildly elevated both in primary tumor and its recurrences despite excessive hormonal activity. We did not perform 18F-FDG PET/CT until second operation, as it was believed to be rather helpful in poorly differentiated tumors and 68Ga-DOTATATE PET/CT was diagnostic. Later, we performed it in search for other metastatic tumors, but the examination showed no tumor spread.
The recommended treatment of thymic NETs regarded radically resectable is thymectomy by median sternotomy or thoracotomy and lymph node dissection (11, 21, 22). According to the last version of the ESMO Guidelines, available literature suggests no benefit from adjuvant therapy in ThCs. The majority of the authors of the Guidelines panel suggest individually discussing eventual postoperative therapies, including RT and/or systemic therapies, balancing the pros and cons only in selected patients with advanced stage R0 or R1-2 resection (22). Data on systemic therapies in thymic NETs are scarce; therefore, they should be discussed in a multidisciplinary expert team in case of morphologically progressive tumors, high tumor burden, or refractory hormonal syndromes. Somatostatin analogs are recommended as the first-line systemic therapy in typical carcinoids (22). We considered the adjuvant therapy with somatostatin analogs; however, due to the low uptake in PET examination and complete resolution of symptoms as well as the radical type of surgical removal, we did not decide to initiate such therapy. Other systemic treatment options include everolimus (second line in typical carcinoids or first line in atypical carcinoids), chemotherapy, peptide receptor radionuclide therapy (PRRT), and interferon-α (22, 23). There is also data on the benefits of combining long-acting lanreotide with temozolomide in progressive thymic NETs (24).
Due to the variable availability of steroid inhibitors during the course of the disease, our patient received three different preparations at each disease relapse. Both ketoconazole and osilodrostat were well tolerated and reduced the hypercortisolism within a few days, but metyrapone caused significant side effects (see below—”Patient’s perspective”), and it was not possible to normalize the cortisol values with this steroid inhibitor. It is worth noting that when using the most recent steroid inhibitor—osilodrostat—we initiated the therapy with a high dose without a previous dose titration. This strategy might be used in the case of severe hypercortisolism and proved effective and safe in our patient (25).
Most commonly, metastases from thymic NET producing ACTH are localized in lymph nodes, bone, lung, pleura, and, less commonly, liver and parotid gland (13). There are very few cases of EAS-related thymic NETs with breast metastases described in the literature, with some histopathological variability (one case related to atypical carcinoid, another to combined large-cell neuroendocrine carcinoma and atypical carcinoid, and third case of neuroendocrine carcinoma). All of them were female patients between 24 and 36 years of age, with mediastinal lymph nodes metastases at the time of presentation; one also had distant metastases to the bones (13–15). Contrary to the reported cases, our patient had typical carcinoid (confirmed by three independent pathologists from different centers) but similarly presented with severe hypercortisolism. It suggests that there is no connection between tumor differentiation and the severity of hypercortisolism. Interestingly, in a review of 661 patients with metastatic NETs from Sweden, there were 20 patients with NETs and breast metastases, and among them only one case of thymic NET (Ki 67 12%), but without EAS. A total of 11 patients with breast metastases had a primary tumor in the small intestine and eight in the lung (16).
Our case underlines the necessity of long-term follow-up in EAS, as the recurrences occurred 5 and 7 years after the initial successful treatment. According to guidelines, follow-up after treatment of thymic NETs should be life-long (22).
The strength of our report is the presentation of a thymic NET with metastasis to the breast, diagnosed and treated with many currently available tools and with a long period of follow-up. The limitation is the low number of other similar cases to compare, which is a consequence of the rarity of this disease.
In conclusion, our case proves that thymic NETs with EAS might present in young patients with well-differentiated character in histopathological examination and severe, life-threatening hypercortisolism despite the small size of the primary lesion. 68Ga-DOTATATE PET/CT is a very helpful tool to localize the tumor. Finally, life-long follow-up should be performed despite complete remission after surgery.
4 Patient’s perspective
The first symptoms that I observed were face edema and mood changes. I rapidly lost muscle mass (approximately 6 kg in 2 weeks), and I was not able to climb stairs, especially with my child’s pram. The most difficult to accept were changes in my appearances—hirsutism, losing hair, changes of my facial features. My sense of pain (for example, during medical procedures) was diminished. Other disruptive symptoms were intensive sweating, increased appetite, thirst, brain fog, and digestive problems. At every relapse, the disease manifestations were fluctuating, all of them intensifying at the same time, which was very difficult for me. Also stress evoked disease symptoms. I experienced a strange feeling of warm during cortisol outbursts.
As for the treatment, I did not tolerate metyrapone well. I had skin rash, anxiety attacks with heart palpitations, and a metallic taste in my mouth. Other drugs (ketoconazole, osilodrostat) were better for me.
After operations of the relapses, the symptoms diminished very quickly, especially the most difficult ones. My blood pressure and glycemia normalized within a few days. Other manifestations, like loss of hair or skin changes, persisted up to 3 months.
Data availability statement
The datasets presented in this article are not readily available because the data are potentially identifiable. Requests to access the datasets should be directed to Aleksandra Zdrojowy-Wełna, aleksandra.zdrojowy-welna@umw.edu.pl.
Ethics statement
This study was exempt from ethical approval procedures being a case report of a single patient who has voluntarily provided oral and written consent to participate in the study and to have her case published for the sake of helping us better understand the clinical picture and the course of thymic neuroendocrine tumors with EAS and share it with the medical community for awareness about it. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributions
AZ-W: Conceptualization, Data curation, Investigation, Methodology, Software, Writing – original draft. MB: Conceptualization, Supervision, Writing – review & editing. JS: Data curation, Investigation, Methodology, Writing – review & editing. AJ-P: Data curation, Investigation, Writing – review & editing. JK-P: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank Prof. Barbara Górnicka and Prof. Michał Jeleń for their collaboration throughout the patient’s treatment.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor AJ declared a past co-authorship with the author MB.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Young J, Haissaguerre M, Viera-Pinto O, Chabre O, Baudin E, Tabarin A. Management of endocrine disease: Cushing’s syndrome due to ectopic ACTH secretion: an expert operational opinion. Eur J Endocrinol. (2020) 182:29–58. doi: 10.1530/EJE-19-0877
5. Ejaz S, Vassilopoulou-Sellin R, Busaidy NL, Hu MI, Waguespack SG, Jimenez C, et al. Cushing syndrome secondary to ectopic adrenocorticotropic hormone secretion: the University of Texas MD Anderson Cancer Center Experience. Cancer. (2011) 117:4381–9. doi: 10.1002/cncr.v117.19
8. Ilias I, Torpy DJ, Pacak K, Mullen N, Wesley RA, Nieman LK. Cushing’s syndrome due to ectopic corticotropin secretion: twenty years’ Experience at the national institutes of health. J Clin Endocrinol Metab. (2005) 90:4955–62. doi: 10.1210/jc.2004-2527
9. Isidori AM, Sbardella E, Zatelli MC, Boschetti M, Vitale G, Colao A, et al. Conventional and nuclear medicine imaging in ectopic cushing’s syndrome: A systematic review. J Clin Endocrinol Metab. (2015) 100:3231–44. doi: 10.1210/JC.2015-1589
10. Liu Q, Zang J, Yang Y, Ling Q, Wu H, Wang P, et al. Head-to-head comparison of 68Ga- DOTATATE PET/CT and 18F-FDG PET/CT in localizing tumors with ectopic adrenocorticotropic hormone secretion: a prospective study. Eur J Nucl Med Mol Imaging. (2021) 48:4386–95. doi: 10.1007/s00259-021-05370-8
11. Gaur P, Leary C, Yao JC. Thymic neuroendocrine tumors: a SEER database analysis of 160 patients. Ann Surg. (2010) 251:1117–21. doi: 10.1097/SLA.0b013e3181dd4ec4
13. Neary NM, Lopez-Chavez A, Abel BS, Boyce AM, Schaub N, Kwong K, et al. Neuroendocrine ACTH-producing tumor of the thymus—Experience with 12 patients over 25 years. J Clin Endocrinol Metab. (2012) 97:2223–30. doi: 10.1210/jc.2011-3355
14. Dzialach L, Wojciechowska-Luzniak A, Maksymowicz M, Witek P. Case report: A challenging case of severe Cushing’s syndrome in the course of metastatic thymic neuroendocrine carcinoma with a synchronous adrenal tumor. Front Endocrinol. (2024). doi: 10.3389/fendo.2024.1399930/full
15. Gaur S, Ayyappan AP, Nahleh Z. Breast metastases from an adrenocorticotropic hormone secreting thymic neuro-endocrine tumor. Breast Dis. (2013) 34:81–6. doi: 10.3233/BD-130354
16. Crona J, Granberg D, Norlén O, Wärnberg F, Stålberg P, Hellman P, et al. Metastases from neuroendocrine tumors to the breast are more common than previously thought. A diagnostic pitfall? World J Surg. (2013) 37:1701–6. doi: 10.1007/s00268-013-2037-2
17. Li B, Yan Z, Huang H. Case report: an unusual case of ectopic ACTH syndrome caused by mediastinal paraganglioma. Front Endocrinol. (2021) 12:790975. doi: 10.3389/fendo.2021.790975
19. Moran CA, Suster S. Neuroendocrine carcinomas (Carcinoid tumor) of the thymus. Am J Clin Pathol. (2000) 114:100–10. doi: 10.1309/3PDN-PMT5-EQTM-H0CD
22. Baudin E, Caplin M, Garcia-Carbonero R, Fazio N, Ferolla P, Filosso PL, et al. Lung and thymic carcinoids: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol. (2021) 32:439–51. doi: 10.1016/j.annonc.2021.01.003
23. Ferolla P, Brizzi MP, Meyer T, Mansoor W, Mazieres J, Do Cao C, et al. Efficacy and safety of long-acting pasireotide or everolimus alone or in combination in patients with advanced carcinoids of the lung and thymus (LUNA): an open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. (2017) 18:1652–64. doi: 10.1016/S1470-2045(17)30681-2
24. Ferolla P, Berruti A, Spada F, Brizzi MP, Ibrahim T, Marconcini R, et al. Efficacy and safety of lanreotide autogel and temozolomide combination therapy in progressive thoracic neuroendocrine tumors (Carcinoid): results from the phase 2 ATLANT study. Neuroendocrinology. (2023) 113:332–42. doi: 10.1159/000526811
25. Fleseriu M, Biller BMK. Treatment of Cushing’s syndrome with osilodrostat: practical applications of recent studies with case examples. Pituitary. (2022) 25:795–809. doi: 10.1007/s11102-022-01268-2
Citation: Zdrojowy-Wełna A, Bolanowski M, Syrycka J, Jawiarczyk-Przybyłowska A and Kuliczkowska-Płaksej J (2025) Case Report: Thymic neuroendocrine tumor with metastasis to the breast causing ectopic Cushing’s syndrome. Front. Oncol. 15:1492187. doi: 10.3389/fonc.2025.1492187
Received: 11 September 2024; Accepted: 31 January 2025;
Published: 25 February 2025.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Cushing’s syndrome, or endogenous hypercortisolemia, is a rare condition that both general practice clinicians and endocrinologists should be prepared to diagnose and treat. Including both the pituitary and adrenal forms of the disease, the Endocrine Society estimates that the disorder affects 10 to 15 people per million every year in the United States. It is more common in women and occurs most often in people between the ages of 20 and 50.
Even though Cushing’s remains a rare disease, cortisol recently made waves at the American Diabetes Association 84th Scientific Session. A highlight of the meeting was the initial presentation of data from the CATALYST trial, which assessed the prevalence of hypercortisolism in patients with difficult-to-control type 2 diabetes (A1c 7.5+).
CATALYST is a prospective, Phase 4 study with two parts. In the prevalence phase, 24% of 1,055 enrolled patients had hypercortisolism, defined as an overnight dexamethasone suppression test (ODST) value greater than 1.8 µg/dL and dexamethasone levels greater than 140 µg/dL. Results of CATALYST’s randomized treatment phase are expected in late 2024.
Elena Christofides, MD, FACE, founder of Endocrinology Associates, Inc., in Columbus, OH, believes the CATALYST results will be a wake-up call for both physicians and patients seeking to advocate for their own health. “This means that nearly 1 in 4 patients with type 2 diabetes have some other underlying hormonal/endocrine dysfunction as the reason for their diabetes, or significant contribution to their diabetes, and they should all be screened,” she said. “All providers need to get comfortable with diagnosing and treating hypercortisolemia, and you need to do it quickly because patients are going to pay attention as well.”
In Dr. Christofides’ experience, patients who suspect they have a hormonal issue may start with their primary care provider or they may self-refer to an endocrinologist. “A lot of Cushing’s patients are getting diagnosed and treated in primary care, which is completely appropriate. But I’ve also met endocrinologists who are uncomfortable diagnosing and managing Cushing’s because it is so rare,” she said. “The important thing is that the physician is comfortable with Cushing’s or is willing to put in the work get comfortable with it.”
According to Dr. Christofides, the widespread popular belief that “adrenal fatigue” is causing millions of Americans to feel sick, tired, and debilitated may be creating barriers to care for people who may actually have Cushing’s. “As physicians, we know that adrenal fatigue doesn’t exist, but we should still be receptive to seeing patients who raise that as a concern,” said Dr. Christofides. “We need to acknowledsalige their lived experience as being very real and it can be any number of diseases causing very real symptoms. If we don’t see these patients, real cases of hypercortisolemia could be left undiagnosed and untreated.”
Dr. Christofides, who also serves as a MedCentral Editor-at-Large, said she reminds colleagues that overnight dexamethasone suppression test (ODST) should always be the first test when you suspect Cushing’s. “While technically a screening test, the ODST can almost be considered diagnostic, depending on how abnormal the result is,” she noted. “But I always recommend that you do the ODST, the ACTH, a.m. cortisol, and the DHEAS levels at the same time because it allows you to differentiate more quickly between pituitary and adrenal problems.”
Dr. Christofides does see a place for 24-hour urine collection and salivary cortisol testing at times when diagnosing and monitoring patients with Cushing’s. “The 24-hour urine is only positive in ACTH-driven Cushing’s, so an abnormal result can help you identify the source, but too many physicians erroneously believe you can’t have Cushing’s if the 24-hour urine is normal,” she explained. “Surgeons tend to want this test before they operate and it’s a good benchmark for resolution of pituitary disease.” She reserves salivary cortisol testing for cases when the patient’s ODST is negative, but she suspects Cushing’s may be either nascent or cyclical.
Surgical resection has long been considered first-line treatment in both the pituitary and adrenal forms of Cushing’s. For example, data shared from Massachusetts General Hospital showed that nearly 90% of patients with microadenomas did not relapse within a 30-year period. A recent study found an overall recurrence rate of about 25% within a 10-year period. When reoperation is necessary, remission is achieved in up to 80% of patients.
As new medications for Cushing’s syndrome have become available, Dr. Christofides said she favors medical intervention prior to surgery. “The best part about medical therapy is you can easily stop it if you’re wrong,” she noted. “I would argue that every patient with confirmed Cushing’s deserves nonsurgical medical management prior to a consideration of surgery to improve their comorbidities and surgical risk management, and give time to have a proper informed consent discussion.”
In general, medications to treat Cushing’s disease rely on either cortisol production blockade or receptor blockade, said Dr. Christofides. Medications that directly limit cortisol production include ketoconazole, osilodrostat (Isturisa), mitotane (Lysodren), levoketoconazole (Recorlev), and metyrapone (Metopirone). Mifepristone (Korlym, Mifeprex) is approved for people with Cushing’s who also have type 2 diabetes to block the effects of cortisol. Mifepristone does not lower the amount of cortisol the body makes but limits its effects. Pasireotide (Signifor) lowers the amount of ACTH from the tumor. Cabergoline is sometimes used off-label in the US for the same purpose.
Following surgery, people with Cushing’s need replacement steroids until their adrenal function resumes, when replacement steroids must be tapered. But Dr. Christofides said she believes that all physicians who prescribe steroids should have a clear understanding of when and how to taper patients off steroids.
“Steroid dosing for therapeutic purposes is cumulative in terms of body exposure and the risk of needing to taper. A single 2-week dose of steroids in a year does not require a taper,” she said. “It’s patients who are getting repeated doses of more than 10 mg of prednisone equivalent per day for 2 or more weeks multiple times per year who are at risk of adrenal failure without tapering.”
Physicians often underestimate how long a safe, comfortable taper can take, per Dr. Christofides. “It takes 6 to 9 months for the adrenals to wake up so if you’re using high-dose steroids more frequently, that will cause the patient to need more steroids more frequently,” she explained. “If you’re treating an illness that responds to steroids and you stop them without tapering, the patient’s disease will flare, and then a month from then to 6 weeks from then you’ll be giving them steroids again, engendering a dependence on steroids by doing so.”
When developing a steroid taper plan for postoperative individuals with Cushing’s (and others), Dr. Christofides suggests basing it on the fact that 5 mg of prednisone or its equivalent is the physiologic dose. “Reduce the dose by 5 mg per month until you get to the last 5 mg, and then you’re going to reduce it by 1 mg monthly until done,” she said. “If a patient has difficulty during that last phase, consider a switch to hydrocortisone because a 1 mg reduction of hydrocortisone at a time may be easier to tolerate.”
Prednisone, hydrocortisone, and the other steroids have different half-lives, so you’ll need to plan accordingly, adds Dr. Christofides. “If you do a slower taper using hydrocortisone, the patient might feel worse than with prednisone unless you prescribe it BID.” She suggests thinking of the daily prednisone equivalent of hydrocortisone as 30 mg to allow for divided dosing, rather than the straight 20 mg/day conversion often used.
What happens after a patient’s Cushing’s has been successfully treated? Cushing’s is a chronic disease, even in remission, Dr. Christofides emphasized. “Once you have achieved remission, my general follow-up is to schedule visits every 6 months to a year with scans and labs, always with the instruction if the patient feels symptomatic, they should come in sooner,” she said.
Magdalena Stasiak,1 Przemysław Witek,2 Emilia Adamska-Fita,1 Andrzej Lewiński1,3
1Department of Endocrinology and Metabolic Diseases, Polish Mother’s Memorial Hospital—Research Institute, Lodz, Poland; 2Department of Internal Medicine, Endocrinology and Diabetes, Medical University of Warsaw; Mazovian Brodnowski Hospital, Warszawa, Poland; 3Department of Endocrinology and Metabolic Diseases, Medical University of Lodz, Lodz, Poland
Correspondence: Magdalena Stasiak, Department of Endocrinology and Metabolic Diseases, Polish Mother’s Memorial Hospital—Research Institute, 281/289 Rzgowska Street, Lodz, 93-338, Poland, Tel +48502049292, Fax +48422711140, Email mstasiak33@gmail.com
Abstract: Cushing’s disease (CD) is the most common cause of endogenous hypercortisolism. Osilodrostat was demonstrated to be efficient in treating CD, and the mean average dose required for CD control was < 11 mg/day. Potential differences in osilodrostat treatment between cortisol-producing adenoma (CPA) and CD have not been reported. The aim of this study was to present two patients with CPA in whom significant differences in the response to therapy compared to CD were found. We demonstrated a case of inverse response of cortisol levels with adrenal tumor progression during the initial dose escalation (Case 1). Simultaneously, severe exaggeration of hypercortisolism symptoms and life-threatening hypokalemia occurred. A further rapid dose increase resulted in the first noticeable cortisol response at a dose of 20 mg/day, and a full response at a dose of 45 mg/day. We also present a case that was initially resistant to therapy (Case 2). The doses required to achieve the first response and the full response were the same as those for Case 1. Our study demonstrated that osilodrostat therapy in patients with CPA may require a different approach than that in CD, with higher doses, faster dose escalation, and a possible initial inverse response or lack of response.
Chronic persistent hypercortisolism is a life-threatening condition that requires effective treatment. Untreated exposure to excessive cortisol secretion leads to severely increased morbidity and mortality due to cardiovascular diseases, thromboembolic events, sepsis, visceral obesity, impairment of glucose metabolism, and dyslipidaea, as well as musculoskeletal disorders, such as myopathy, osteoporosis, and skeletal fractures. Moreover, neuropsychiatric disorders, such as impairment of cognitive function, depression, or mania, as well as impairment of reproductive function can frequently occur.1,2 Cushing’s disease (CD) – a disorder caused by a pituitary adenoma secreting adrenocorticotropic hormone (ACTH) – is the most common cause of hypercortisolism. Cushing’s syndrome (CS) includes all other causes of cortisol excess, including ectopic ACTH production as well as direct cortisol overproduction by adrenal adenoma (cortisol-producing adenoma [CPA]) or adrenocortical carcinoma (ACC). Approximately 10% of hypercortisolism cases result from CPA. The first line therapy is a surgical resection of the tumor, which is the source of hormone excess. However, in many patients surgery is not fully efficient and other therapies are required to reduce cortisol levels. Additionally, due to severe cardiovascular complications and unstable DM, the surgical approach sometimes entails unacceptable risk and it is frequently postponed until cortisol levels are lowered. Pharmacotherapy with steroidogenesis inhibitors reduces cortisol levels and improves the symptoms of hypercortisolism.1,2 As CD is the most common cause of cortisol excess, most studies have focused on the efficacy and safety of novel steroidogenesis inhibitors, including patients with CD only.3–6 This is exactly the case with osilodrostat – a new potent inhibitor of 11β-hydroxylase.3–6 More data are available for metyrapone efficacy and safety in CSA,7 as the drug has been available much longer than osilodrostat. A study by Detomas et al, which reported results of comparison of efficacy of metyrapone and osilodrostat, included 4 patients with adrenal CS, among whom one CPA patient was treated with osilodrostat.8 Osilodrostat is approved in the United States to treat CD in patients in whom pituitary surgery was not curative or is contraindicated.9 In Poland, osilodrostat therapy is available for patients with all kinds of endogenous hypercortisolism not curative with other approaches, within a national program of emergency access to drug technologies.10 Reports on osilodrostat application in CPA are highly valuable as data on potential differences in the treatment regimens between CD and CPA are scarce.
Here, we present two patients with CPA in whom the response and doses of osilodrostat were different from those reported in patients with CD. The main purpose of this study was to demonstrate that the efficacy of osilodrostat in CPA is high, although initial resistance to treatment or even deterioration of hypercortisolism can occur during the application of lower doses of the drug.
Materials and Methods
Study Design and Patients
We retrospectively analyzed medical files of two consecutive patients with CPA treated with osilodrostat. The analysis included medical history, laboratory and imaging results as well as a detailed reports of adverse events.
Laboratory and Imaging Procedures
Serum cortisol and ACTH levels were measured by electrochemiluminescence immunoassay (ECLIA) using a Cobas e601 analyzer (Roche Diagnostics, Indianapolis, IN, USA). UFC excretion was measured by chemiluminescent microparticle immunoassay (CMIA) using an Abbott Architect ci4100 analyzer (Abbott, Abbott Park, IL, USA). Cross-reactivity with 11-deoxycortisol for this method is very low (2.1% according to the manufacturer’s data). Potassium levels were measured by ion-selective electrode potentiometry using a Beckman Coulter DxC 700 AU Chemistry Analyzer (Beckman Coulter, Brea, CA, USA). Computed tomography (CT) imaging was performed using a Philips Ingenuity Core 128 system (Philips, the Netherlands).
Ethics Procedures
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patients for publication of this paper. The approval of Institutional Ethics Committee was obtained to publish the case details (approval code KB 33/2023).
Presentation of the Cases
Case 1
A 51-year-old female was referred to our department in November 2021 because of CPA, disqualified from surgery because of severe hypertension with a poor response to antihypertensive therapy and uncontrolled DM despite high doses of insulin. Additionally, the patient presented with hyperlipidemia and severe obesity (BMI=50.7 kg/m2), gastritis, depression, and osteoarthritis. On admission, she complained of a tendency to gain weight, fragile skin that bruised easily, difficulty with wound healing, susceptibility to infections, and insomnia. Physical examination revealed a moon face with plethora, a buffalo hump, central obesity with proximal muscle atrophy, and purple abdominal striae.
The CPA diagnosis was initially made two years earlier, but the patient did not qualify for surgery due to a hypertensive crisis. Soon after this episode, the SARS-CoV-2 pandemic began, and the patient was afraid of visiting any medical center because her son had died of COVID-19. Therefore, she was referred to our center for life-threatening hypercortisolism two years later.
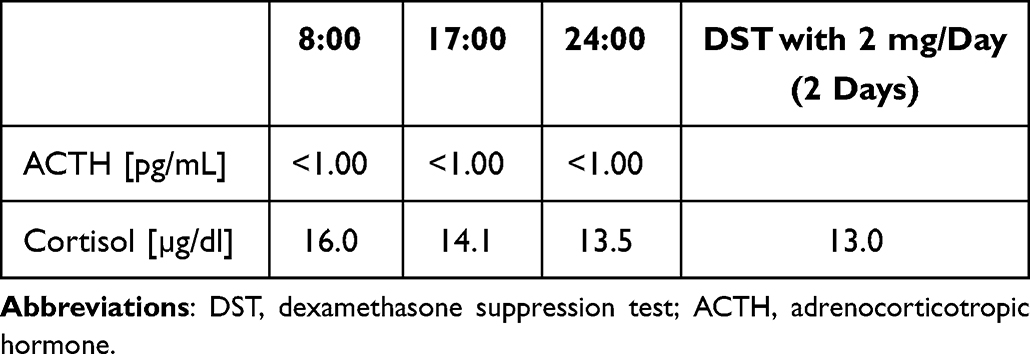
At the time of admission, computed tomography (CT) imaging revealed a right adrenal tumor of 34x24x37mm, with a basal density of 21 HU and a contrast washout rate typical for adenomas (83%). The size and CT characteristics were identical as they were two years earlier. High serum cortisol levels, undetectable ACTH concentrations, and a lack of physiological diurnal rhythm of cortisol secretion were observed (Table 1). Urinary free cortisol (UFC) excretion was 310 µg/24 h, with an upper normal limit (UNL) of 176 µg/24 h. No cortisol suppression was achieved in high-dose dexamethasone suppression test (DST) (Table 1). Other adrenal-related hormonal parameters were within normal ranges, with values as follows: DHEA-S 42.68 µg/dl, aldosterone 3.24 ng/mL, and renin 59.14 µIU/mL.
Table 1 Laboratory Results Before Osilodrostat Therapy – Case 1
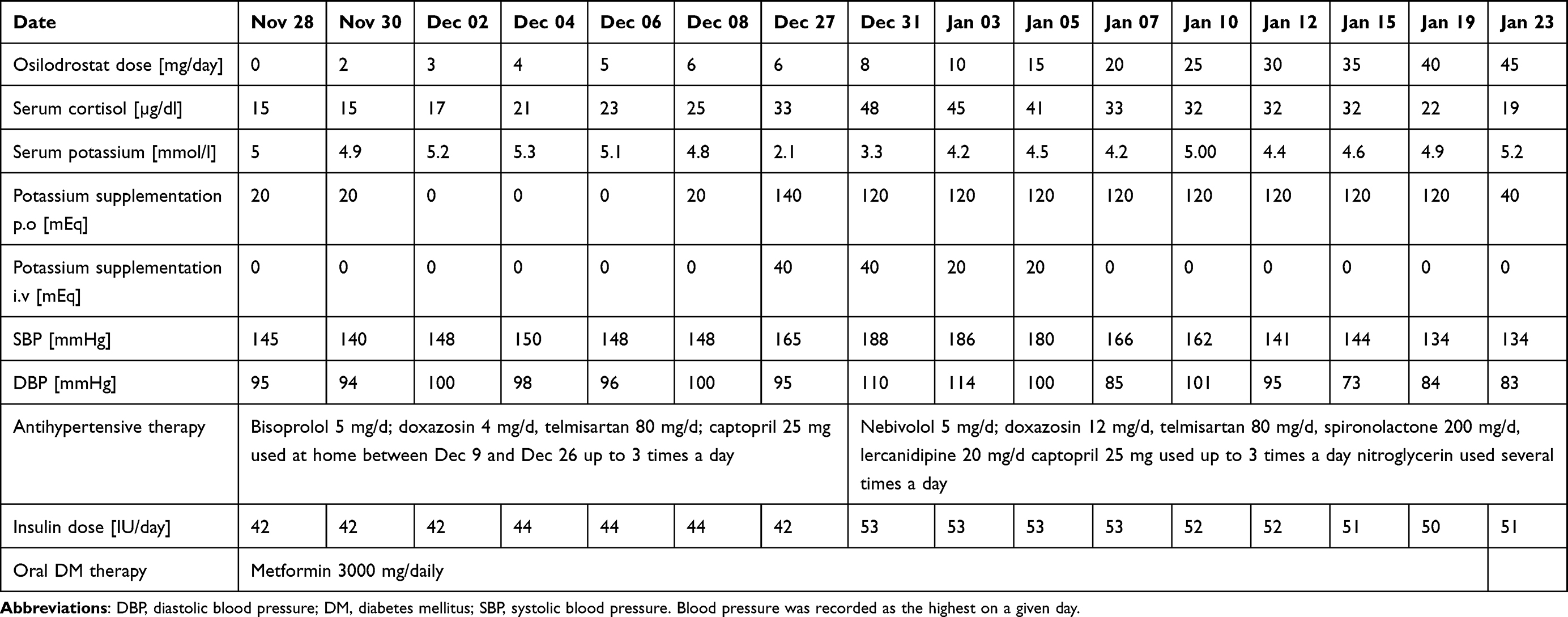
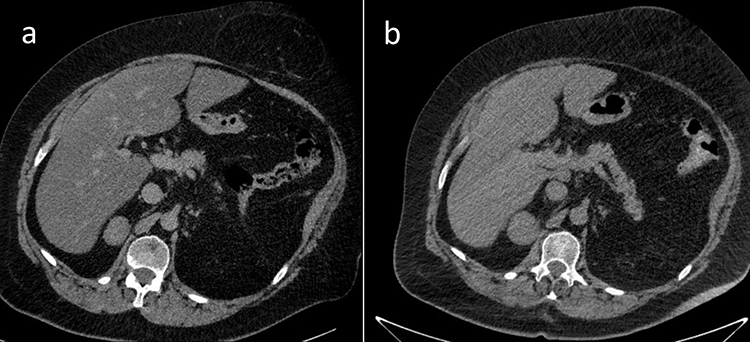
Due to multiple severe systemic complications, including uncontrolled hypertension, decompensated DM, and cardiac insufficiency, treatment with osilodrostat was introduced for life-saving pre-surgical management. Osilodrostat was started at a dose of 1 mg twice daily and gradually increased to 6 mg per day with actually an inverse response of serum cortisol level. The late-night cortisol level increased from 16 µg/dl to 25 µg/dl. As the full effect of the osilodrostat dose can occur even after a few weeks, the patient was discharged from hospital and instructed to contact her attending doctor immediately if any health deterioration was noticed. In the case of improvement in the patient’s condition, the next hospitalization was planned 3 weeks later. After three weeks of no contact with the patient, she was readmitted to our department with life-threatening escalation of hypercortisolism, severe hypokalemia, and further deterioration of hypertension, DM, cardiac insufficiency, dyspnea, and significant edemas, including facial edema. Treatments of hypertension, cardiac insufficiency, and DM were intensified, as presented in Table 2. Despite active potassium supplementation, life-threatening hypokalemia of 2.1 mmol/l occurred. Previously observed depression was exaggerated with severe anxiety and fear of death. The dose of osilodrostat was increased to 8 mg/day, and after three days of treatment a further elevation of serum cortisol was found, with an increase in UFC up to 9 × UNL (1546.2 µg/24 h). Due to an entirely unexpected inverse cortisol response, CT imaging was performed and revealed progression of the adenoma size to 39 × 36 × 40 mm, with a slight increase in density up to 27 HU as compared to the previous CT scan performed a month earlier (Figure 1).
Table 2 Changes in the Most Important Parameters During Osilodrostat Therapy – Case 1
Figure 1 Progression of the adrenal adenoma size during the initial doses of osilodrostat: (a) CT scan directly before osilodrostat therapy – solid nodule 34x24x37 mm, basal density 21 HU; (b) CT scan during treatment with 8 mg of osilodrostat daily – solid nodule 39x36x40 mm, basal density of 27 HU.
Considering the extremely high risk associated with such a rapid cortisol increase and related complications, decision of fast osilodrostat dose escalation was made. The dose was increased by 5 mg every other day, up to 45 mg per day, and, finally, a gradual decrease in the cortisol level (Table 2) was achieved, with UFC normalization to 168 µg/24 h. During dose escalation, no deterioration in the adverse effects (AEs) of osilodrostat was observed. Conversely, hypokalemia gradually improved despite a simultaneous reduction in potassium supplementation (Table 2). Facial edema decreased and the level of anxiety improved significantly. The course of hypertension severity as well as a summary of the main parameters controlled during treatment and the medications used are presented in Table 2. As soon as the cortisol level normalized, the patient was referred for surgery and underwent right adrenalectomy without any complications. Histopathology results confirmed a benign adenoma of the right adrenal gland (encapsulated, well-circumscribed tumor consisting of lipid-rich cells with small and uniform nuclei, mostly with eosinophilic intracytoplasmic inclusions). After surgery, hydrocortisone replacement therapy was administered. A few days after surgery, blood pressure and glucose levels gradually decreased, and the patient required reduction of antihypertensive and antidiabetic medications. After 22 months of follow-up, the patient’s general condition is good with no signs of recurrence. Antidepressant treatment is no longer required in this patient. Body mass index was significantly reduced to 40 kg/m2. The antihypertensive medication was completely discontinued, and the glucose level is controlled only with metformin. The patient still requires hydrocortisone substitution at a dose of 30 mg/day.
Case 2
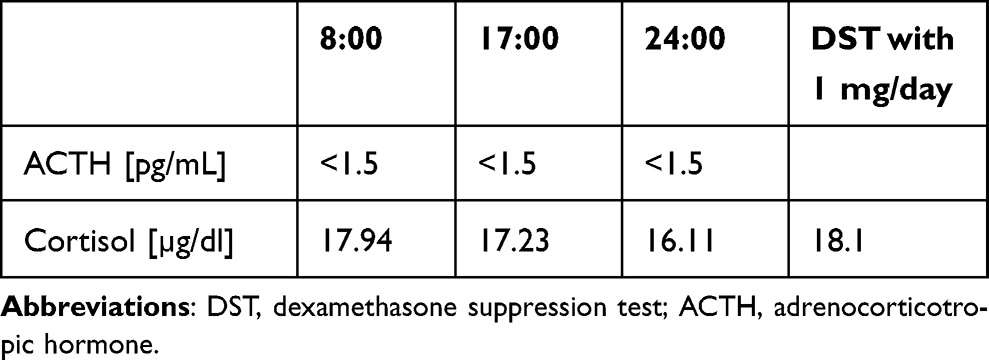
A 39-year-old female was referred to our department in November 2022 with a diagnosis of CPA and unstable hypertension, for which surgery was contraindicated. The patient was unsuccessfully treated with triple antihypertensive therapy (telmisartan 40 mg/day, nebivolol 5 mg/day, and lercanidipine 20 mg/day). The patient reported weight gain, muscle weakness, acne, fragile skin that bruised easily, and secondary amenorrhea. Other comorbidities included gastritis, hypercholesterolemia, and osteoporosis. Physical examination revealed typical signs of Cushing’s syndrome, such as abnormal fat distribution, particularly in the abdomen and supraclavicular fossae, proximal muscle atrophy, moon face, and multiple hematomas. A lack of a serum cortisol diurnal rhythm with high late-night serum cortisol and undetectable ACTH levels was found (Table 3). The short DST revealed no cortisol suppression (Table 3), and the UFC result was 725 µg/24 h, which exceeded the UNL more than four times. The serum levels of renin, aldosterone, and 24-h urine fractionated metanephrines were within the normal ranges. Computed tomography imaging revealed a left adrenal gland tumor measuring 25 × 26 × 22 mm, with a basal density of 32 HU and a washout rate typical for adenoma (76%).
Table 3 Laboratory Results Before Osilodrostat Therapy – Case 2
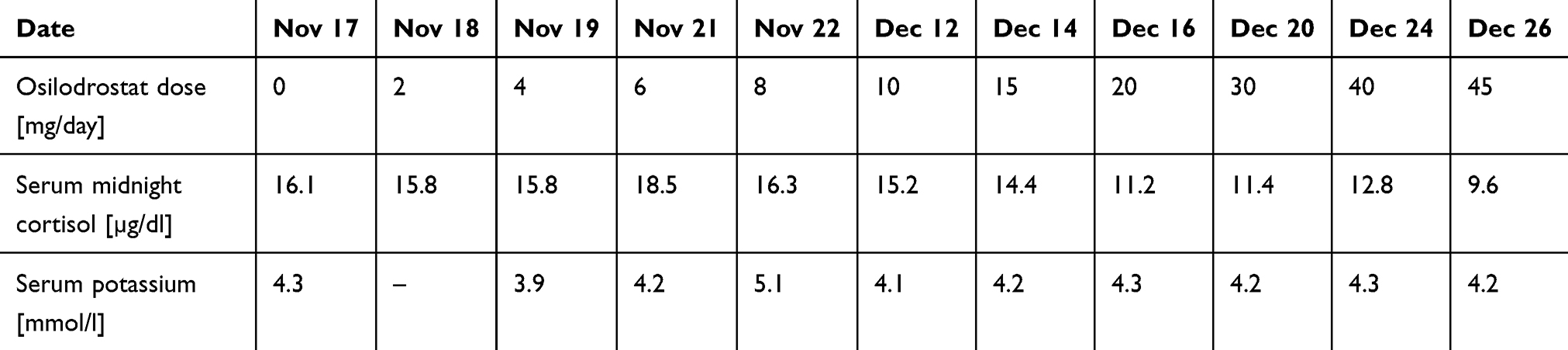
Osilodrostat therapy was administered for preoperative management. The initial daily dose was 2 mg/day, increased gradually by 2 mg every day with no serum cortisol response (late night cortisol levels 15.8–18.5 µg/dl) and no AEs of the drug (Table 4). After the daily dose of osilodrostat reached 10 mg, it was escalated by 5 mg every other day, initially with no serum cortisol reduction. The dose was increased to 45 mg daily (with the lowest detected late-night serum cortisol of 9.6 µg/dl) (Table 4).
Table 4 Changes in the Most Important Parameters During Osilodrostat Therapy – Case 2
After a week of administration of 45 mg daily, UFC normalization was achieved. Despite rapid dose escalation, no AEs were observed during the entire therapy period. Potassium levels were normal without any supplementation (the lowest detected serum potassium level was 3.9 mmol/l; all other results were over 4.0 mmol/l) (Table 4). After UFC normalization, left adrenalectomy was performed without complications. Histopathological examination revealed benign adrenal adenoma. Antihypertensive therapy was reduced only to 2.5 mg of nebivolol daily. The patient’s general condition improved significantly. Currently, hydrocortisone replacement therapy is administered at a dose of 15 mg/day.
Discussion
Osilodrostat is a novel potent steroidogenesis inhibitor whose efficacy and safety have been thoroughly analyzed in clinical trials of patients with CD, the most common cause of endogenous hypercortisolism. No clinical trial of osilodrostat therapy in CPA has been performed, as this disease constitutes only 10% of all cases of endogenous hypercortisolism. Moreover, osilodrostat is not approved by the FDA for hypercortisolism conditions other than CD.9 Therefore, data on potential differences in the treatment regimen are lacking.
During the course of already reported trials in CD, osilodrostat doses were escalated slowly, every 2–3 weeks,3,5,6 with an excellent response to quite low doses of the drug.3–6 In the LINC 2 extension study the median average dose was 10.6 mg/day,5 while in the LINC 3 extension study and the LINC 4 study it was 7.4 mg/day and 6.9 mg/day, respectively.4,6 In most cases, a significant decrease of hypercortisolism was reported with the low doses of osilodrostat (4 or 10 mg/day). Moreover, some patients received 1 mg/day or even 1 mg every other day, with a good response.6 Even in rare cases of CD in whom initial short-term etomidate therapy was given at the beginning of osilodrostat therapy, due to highly severe life-threatening symptoms of hypercortisolism, the final effective dose of osilodrostat was much lower than that in our patients with CPA (25 mg/day vs 45 mg/day) and no increase of cortisol level was observed.11
It should be underlined that many cases of adrenal insufficiency during osilodrostat therapy in patients with CD have been reported,3–6,12,13 and – therefore – low initial dose with slow gradual dose escalation is recommended in patients with CD.1,6,13
In the cases presented here, CPA led to severe hypercortisolism, the complications of which constituted contraindications for surgery. Therefore, osilodrostat therapy was introduced as a presurgical treatment. In Case 1, the therapy was started at low doses according to the approved product characteristics.14 Due to the severity of hypertension, which was uncontrolled despite of active antihypertensive therapy, as well as to unstable DM, the doses were increased faster than recommended. Surprisingly, we immediately observed a gradual increase in hypercortisolism, in both serum cortisol levels and the UFC, with simultaneous burst of complications related to both hypercortisolism itself and 11β-hydroxylase inhibition. Life-threatening episodes of hypertensive crisis responded poorly to standard therapies. Severe exaggeration of cardiac insufficiency could probably be related to these episodes as well as to deep hypokalemia, which occurred despite potassium supplementation. Hypokalemia is a typical complication of treatment with 11β-hydroxylase inhibitors due to the accumulation of adrenal hormone precursors. However, Patient 1 required much higher doses of potassium supplementation, both parenteral and oral, than ever described during osilodrostat therapy.3–6,13 The dose of 20 mg/day of osilodrostat was the first one which led to noticeable cortisol reduction and a decrease in systolic blood pressure (SBP) to below 170 mmHg. Surprisingly, instead of the expected deterioration of hypokalemia, parenteral potassium administration could be stopped with an osilodrostat dose of 20 mg/day and oral supplementation was gradually reduced simultaneously with osilodrostat dose escalation. The reason why such severe hypokalemia occurred with low doses of osilodrostat and did not deteriorate further seems complex. One possible reason is the administration of high doses of potassium-saving antihypertensive drugs such as spironolactone and the angiotensin II receptor antagonist telmisartan. Additionally, one can consider other possible mechanisms, such as downregulation of the receptors of deoxycorticosterone (DOC) or other adrenal hormone precursors. However, this hypothesis requires further research and confirmation. Such an improvement of the potassium level during osilodrostat dose escalation was previously demonstrated in a patient with CD.11 Interestingly, in our Patient 2, no potassium supplementation was required during the whole time of osilodrostat therapy, although the doses were increased intensively up to the finally effective dose, which was the same (45 mg/day) as for Patient 1. In Patient 2, no actual response to doses lower than 20 mg/day was observed. UFC normalization was achieved after a week of administration of 45 mg/day, five weeks from the beginning of therapy. Although UFC normalization is not always required in pre-surgical treatment, clinical symptoms significantly improved in our patients only after the UFC upper normal level was achieved.
The present paper is one of only a few reports focused on osilodrostat therapy in CPA, and the only one presenting a different therapy course as compared to patients with CD. No case of CPA resistance to low doses of osilodrostat has been described. It should be underlined that in our report “low doses” of osilodrostat were higher than the average mean doses of osilodrostat used in clinical trials in patients with CD.3–6 Therefore, they should not generally be considered low but only much lower than those which were effective in our patients. Malik and Ben-Shlomo presented a case of CPA treated with osilodrostat, with an immediate decrease in cortisol level at 4 mg/day and adrenal insufficiency symptoms after dose escalation to 8 mg/day.15 Similar to our two cases, their patient was a middle-aged female with normal results of all other adrenal parameters, such as renin, angiotensin, or metanephrine levels. However, a CT scan was not performed (or presented), while magnetic resonance imaging revealed an indeterminate adrenal gland mass without a typical contrast phase/out-of-phase dropout for adenoma.15 Therefore, different morphology of cortisol-secreting adrenal tumor can potentially be considered a reason of the different response to treatment. Tanaka et al performed a multicenter study on the efficacy and safety of osilodrostat in Japanese patients with non-CD Cushing’s syndrome.16 Five patients with CPA were included in the study, and none of them required osilodrostat doses higher than 10 mg/day to achieve UFC normalization. However, most of the patients presented by Tanaka et al were previously treated with metyrapone,16 whereas both of our patients were treatment-naive. Previous metyrapone therapy may be considered as a potential reason of better response to osilodrostat. This hypothesis was confirmed in the quoted study by Tanaka et al, who demonstrated that at week 12 the median percent changes in the mUFC values were higher in patients previously treated with metyrapone (–98.97%) than in treatment-naive cases (–86.65%).16 Detomas et al performed a comparison of efficacy and safety of osilodrostat and metyrapone, with one CPA patients included in a group treated with osilodrostat, however no data on a dose required for a disease control are available separately for this particular patient.8 To the best of our knowledge, no more CPA cases have been described and therefore no further comparison is available.
Higher doses of osilodrostat were administered to a group of seven patients with hypercortisolism due to adrenocortical carcinoma (ACC) presented by Tabarin et al.17 A full control of hypercortisolism was achieved in one patient for each dose of 4, 8, 10, and 20 mg/day, and in three patients treated with 40 mg/day.17 These patients, however received other therapies including mitotane and chemotherapy, which can significantly modify the response to osilodrostat.
Several authors have reported the phenomenon of a partial or total loss of response to osilodrostat.5,16,17 In such cases, a response to treatment was initially achieved and then lost during treatment with the same dose. A further increase in osilodrostat dose usually resulted in the response resumption.5,16,17 Such a situation could not be suspected in either of our cases.
The presented cases provide a novel insight into modalities of treatment with osilodrostat in patients with CPA and demonstrate for the first time that an inverse cortisol response is possible in CPA cases, especially those with a higher CT density of adrenal adenoma. Such a situation should not be considered a contraindication to dose escalation. Conversely, the dose should be increased more intensively so as to achieve the initial efficacy threshold, which was 20 mg/day in both of our patients. The fully efficient dose that allowed UFC normalization was more than twice as high (45 mg/day in both cases). A similar approach should be applied in patients who do not respond to lower doses, such as Patient 2. The safety of osilodrostat therapy is strictly individual and not dose dependent in patients with CPA. Adverse events, including hypokalemia, severe hypertension, and edema, can be of life-threatening severity or may not occur regardless of the dose. Moreover, AEs of high severity may decrease with osilodrostat dose escalation. Our study demonstrated that osilodrostat is efficient and can be used in patients with CPA as a pre-surgical therapy if surgery is contraindicated due to hypercortisolism complications.
Our study presented two cases of CPA treated with osilodrostat, and a small size of our group is the main limitation of this report. Future research is required to confirm our observations.
Conclusion
In some patients with CPA, the doses of osilodrostat required for disease control can be much higher than those previously reported. Acceleration of the dose increase can be fast, and the risk of overdosing, adrenal insufficiency, and later necessity of dose reduction seem to be much lower than it could be expected. Low initial doses (<20 mg/day in our study) can be entirely ineffective or can even cause exacerbation of hypercortisolism, whereas high doses (45 mg/day in the present study) are efficient in pre-surgery UFC normalization. AEs associated with osilodrostat can be rapid, with severe hypokalemia despite active potassium supplementation, or may not occur even if high doses of osilodrostat are applied. Therefore, close monitoring for potential AEs is necessary.
Acknowledgments
The abstract included some parts of this paper was presented at the European Congress of Endocrinology ECE2023 as a rapid communication. The abstract was published in the Endocrine Abstracts Vol. 90 [https://www.endocrine-abstracts.org/ea/0090/].
Funding
The publication of this report was financially supported by the statutory funds of the Polish Mother’s Memorial Hospital – Research Institute, Lodz, Poland.
Disclosure
Professor Przemysław Witek reports personal fees from Investigator in the clinical trials paid by Novartis and Recordati Rare Diseases, outside the submitted work; lectures fees from Recordati Rare Diseases, Strongbridge, IPSEN. The authors report no other conflicts of interest in this work.
References
1. Fleseriu M, Auchus R, Bancos I, et al. Consensus on diagnosis and management of Cushing’s disease: a guideline update. Lancet Diabetes Endocrinol. 2021;9(12):847–875. doi:10.1016/S2213-8587(21)00235-7
2. Pivonello R, Isidori AM, De Martino MC, et al. Complications of Cushing’s syndrome: state of the art. Lancet Diabetes Endocrinol. 2016;4(7):611–629. doi:10.1016/S2213-8587(16)00086-3
3. Pivonello R, Fleseriu M, Newell-Price J, et al. Efficacy and safety of osilodrostat in patients with Cushing’s disease (LINC 3): a multicentre Phase III study with a double-blind, randomised withdrawal phase. Lancet Diabetes Endocrinol. 2020;8(9):48–761. doi:10.1016/S2213-8587(20)30240-0
4. Fleseriu M, Newell-Price J, Pivonello R, et al. Long-term outcomes of osilodrostat in Cushing’s disease: LINC 3 study extension. Eur J Endocrinol. 2022;187(4):531–541. doi:10.1530/EJE-22-0317
5. Fleseriu M, Biller BMK, Bertherat J, et al. Long-term efficacy and safety of osilodrostat in Cushing’s disease: final results from a Phase II study with an optional extension phase (LINC 2). Pituitary. 2022;25(6):959–970. doi:10.1007/s11102-022-01280-6
6. Gadelha M, Bex M, Feelders RA, et al. Randomized trial of osilodrostat for the treatment of Cushing disease. J Clin Endocrinol Metab. 2022;107(7):e2882–e2895. doi:10.1210/clinem/dgac178
7. Daniel E, Aylwin S, Mustafa O, et al. Effectiveness of metyrapone in treating cushing’s syndrome: a retrospective multicenter study in 195 patients. J Clin Endocrinol Metab. 2015;100(11):4146–4154. doi:10.1210/jc.2015-2616
8. Detomas M, Altieri B, Deutschbein T, et al. Metyrapone versus osilodrostat in the short-term therapy of endogenous cushing’s syndrome: results from a single center cohort study. Front Endocrinol. 2022;13:903545. doi:10.3389/fendo.2022.903545
11. Dzialach L, Sobolewska J, Respondek W, et al. Cushing’s syndrome: a combined treatment with etomidate and osilodrostat in severe life-threatening hypercortisolemia. Hormones. 2022;21(4):735–742. doi:10.1007/s42000-022-00397-4
12. Ekladios C, Khoury J, Mehr S, et al. Osilodrostat-induced adrenal insufficiency in a patient with Cushing’s disease. Clin Case Rep. 2022;10(11):e6607. doi:10.1002/ccr3.6607
13. Fleseriu M, Biller BMK. Treatment of Cushing’s syndrome with osilodrostat: practical applications of recent studies with case examples. Pituitary. 2022;25(6):795–809. doi:10.1007/s11102-022-01268-2
15. Malik RB, Ben-Shlomo A. Adrenal cushing’s syndrome treated with preoperative osilodrostat and adrenalectomy. AACE Clin Case Rep. 2022;8(6):267–270. doi:10.1016/j.aace.2022.10.001
16. Tanaka T, Satoh F, Ujihara M, et al. A multicenter, Phase 2 study to evaluate the efficacy and safety of osilodrostat, a new 11β-hydroxylase inhibitor, in Japanese patients with endogenous Cushing’s syndrome other than Cushing’s disease. Endocr J. 2020;67(8):841–852. doi:10.1507/endocrj.EJ19-0617
17. Tabarin A, Haissaguerre M, Lassole H, et al. Efficacy and tolerance of osilodrostat in patients with Cushing’s syndrome due to adrenocortical carcinomas. Eur J Endocrinol. 2022;186(2):K1–K4. doi:10.1530/EJE-21-1008
In a recent study published in Hypertension Research, scientists examine the endocrine causes of hypertension (HTN) and investigate the efficacy of treatments to alleviate HTN.
What is HTN?
About 30% of the global population is affected by HTN. HTN is a modifiable cardiovascular (CV) risk factor that is associated with a significant number of deaths worldwide.
There are two types of HTN known as primary and secondary HTN. As compared to primary HTN, secondary HTN causes greater morbidity and mortality.
The most common endocrine causes of HTN include primary aldosteronism (PA), paragangliomas and pheochromocytomas (PGL), Cushing’s syndrome (CS), and acromegaly. Other causes include congenital adrenal hyperplasia, mineralocorticoid excess, cortisol resistance, Liddle syndrome, Gordon syndrome, and thyroid and parathyroid dysfunction.
What is PA?
PA is the most common endocrine cause of hypertension, which is associated with excessive aldosterone secretion by the adrenal gland and low renin secretion. It is difficult to estimate the true prevalence of PA due to the complexity of its diagnosis.
Typically, the plasma aldosterone-to-renin ratio (ARR) is measured to diagnose PA. The diagnosis of PA can also be confirmed using other diagnostic tools like chemiluminescent enzyme immunoassays (CLEIAs) and radio immune assay (RIA).
Continuous aldosterone secretion is associated with organ damage due to chronic activation of the mineralocorticoid (MR) receptor in many organs, including fibroblasts and cardiomyocytes. An elevated level of aldosterone causes diastolic dysfunction, endothelial dysfunction, left ventricular hypertrophy, and arterial stiffness.
Increased aldosterone secretion also leads to obstructive sleep apnea and increases the risk of osteoporosis. This is why individuals with PA are at a higher risk of cardiovascular events (CVDs), including heart failure, myocardial infarction, coronary artery disease, and atrial fibrillation.
PA is treated by focusing on normalizing potassium and optimizing HTN and aldosterone secretion. Unilateral adrenalectomy is a surgical procedure proposed to treat PA.
Young patients who are willing to stop medication are recommended surgical treatment. The most common pharmaceutical treatment for PA includes mineralocorticoid receptor antagonists such as spironolactone and eplerenone.
Pheochromocytomas and paragangliomas
PGL are tumors that develop at the thoracic-abdominal-pelvic sympathetic ganglia, which are present along the spine, as well as in the parasympathetic ganglia located at the base of the skull. The incidence rate of PGL is about 0.6 for every 100,000 individuals each year. PGL tumors synthesize excessive catecholamines (CTN), which induce HTN.
Some of the common symptoms linked to HTN associated with PGL are palpitations, sweating, and headache. PGL can be diagnosed by determining metanephrines (MN) levels, which are degraded products of CTN. Bio-imaging tools also play an important role in confirming the diagnosis of PGL.
Excessive secretion of CTN increases the risk of CVDs, including Takotsubo adrenergic heart disease, ventricular or supraventricular rhythm disorders, hypertrophic obstructive or ischaemic cardiomyopathy, myocarditis, and hemorrhagic stroke. Excessive CTN secretion also causes left ventricular systolic and diastolic dysfunction.
Typically, PGL treatment is associated with surgical procedures. Two weeks before the surgery, patients are treated with alpha-blockers. For these patients, beta-blockers are not used as the first line of treatment without prior use of alpha-adrenergic receptors.
Patients with high CTN secretion are treated with metyrosine, as this can inhibit tyrosine hydroxylase. Hydroxylase converts tyrosine into dihydroxyphenylalanine, which is related to CTN synthesis.
What is CS?
CS, which arises due to persistent exposure to glucocorticoids, is a rare disease with an incidence rate of one in five million individuals each year. The most common symptoms of CS include weight gain, purple stretch marks, muscle weakness, acne, and hirsutism. A high cortisol level causes cardiovascular complications such as HTN, hypercholesterolemia, and diabetes.
CS is diagnosed based on the presence of two or more biomarkers that can be identified through pathological tests, such as salivary nocturnal cortisol, 24-hour urinary-free cortisol, and dexamethasone suppression tests.
CS is treated through surgical procedures based on the detected lesions. Patients with severe CS are treated with steroidogenic inhibitors, such as metyrapone, ketoconazole, osilodrostat, and mitotane. Pituitary radiotherapy and bilateral adrenalectomy are performed when other treatments are not effective.
Acromegaly
Acromegaly arises due to chronic exposure to growth hormone (GH), leading to excessive insulin-like growth factor 1 (IGF1) synthesis. This condition has a relatively higher incidence rate of 3.8 million person-years. Clinical symptoms of acromegaly include thickened lips, widened nose, a rectangular face, prominent cheekbones, soft tissue overgrowth, or skeletal deformities.
Prolonged exposure to GH leads to increased water and sodium retention, insulin resistance, reduced glucose uptake, and increased systemic vascular resistance. These conditions increase the risk of HTN and diabetes in patients with acromegaly. Acromegalic patients are also at a higher risk of cancer, particularly those affecting the thyroid and colon.
Acromegaly is diagnosed using the IGF1 assay, which determines IGF1 levels in serum. After confirming the presence of high IGF1 levels, a GH suppression test must be performed to confirm the diagnosis. Bioimaging is also conducted to locate adenoma.
Acromegaly is commonly treated through surgical procedures. Patients who refuse this line of treatment are treated with somatostatin receptor ligands, growth hormone receptor antagonists, dopaminergic agonists, or radiotherapy.
Journal reference:
De Freminville, J., Amar, L., & Azizi, M. (2023) Endocrine causes of hypertension: Literature review and practical approach. Hypertension Research; 1-14. doi:10.1038/s41440-023-01461-1





 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at 