Introduction
Transsphenoidal surgery is the primary treatment for patients with Cushing disease (CD). This study assessed the surgical and endocrinologic outcomes of patients with CD following endoscopic pituitary surgery using strict biochemical criteria to guide surveillance in patients not achieving early remission.
Methods
The medical records of all patients with CD who underwent endoscopic transsphenoidal surgery at a single institution between 2004 and 2025 were reviewed. Remission was defined as a fasting serum cortisol level <50 nmol/L (1.8 μg/dL) either basal or after 1 mg dexamethasone.
Results
A total of 125 patients were diagnosed with CD and had a primary endoscopic transsphenoidal surgery during the study period (median age 48 years [range: 14–79 years; M:F 93:32). Fifty-seven patients (45.6%) had a microadenoma, 41 (32.8%) had a macroadenoma, and 26 (20.8%) had no demonstrable focal lesion on pituitary magnetic resonance imaging (MRI) (MRI-negative CD). The median length of follow-up was 3.1 years (range: 1 month to 16.7 years). Initial remission rates 3 months after surgery were: 72.0% for patients with MRI-negative CD, 77.2% for microadenomas, and 48.7% for macroadenomas. Age, male sex, MRI-negative, and single operation were predictors of remission. Patients who achieved remission at 3 months were significantly more likely to be in remission at last follow-up after accounting for patient and tumor characteristics. The 5-year recurrence rate following remission was 6.9%.
Conclusion
Endoscopic transsphenoidal surgery is an effective first-line treatment for patients with CD but a significant minority will relapse. Close biochemical surveillance of patients who fail to achieve remission may support the use of early adjuvant radiotherapy.
Key words
Cushing disease
Endoscopic transsphenoidal surgery
Remission
Abbreviations
CD
Cushing’s Disease
CSF
Cerebrospinal fluid
DI
Diabetes insipidus
MRI
Magnetic Resonance Imaging
Introduction
Cushing disease (CD) is a rare endocrine disease caused by the circulation of excess cortisol due to hypersecretion of adrenocorticotrophic hormone from a pituitary adenoma. The annual incidence of CD is estimated to be between 1.2 and 2.4 million cases per year1, 2, 3 although it may be higher in selected patient populations such as those with poorly controlled diabetes and young patients with osteoporosis or hypertension.4 Untreated CD is associated with a very poor prognosis and a significantly reduced 5-year survival mandating prompt and effective treatment.5 Nevertheless, long-term management of patients with CD remains challenging.
In most cases of CD, the pituitary adenoma is benign and excellent remission rates have been reported with surgical treatment.6, 7, 8 Comparable remission rates of around 80% have been reported with both microscopic and endoscopic transsphenoidal pituitary surgery,7,8 however the basal serum cortisol level used to define remission varies significantly in the literature (50–138 nmol/L). Several previous studies have also excluded macroadenomas and invasive tumors from longitudinal analysis. As such, there is a paucity of long-term clinical data for an unselected population undergoing endoscopic transsphenoidal pituitary surgery for CD. Furthermore, there is little evidence concerning the optimal management of patients who fail to enter complete biochemical remission (basal serum cortisol level <50 nmol/L [1.8 μg/dL]) following their initial surgical treatment.
The aim of this study was to assess the treatment pathway and long-term outcomes of consecutive patients treated at a regional treatment center over a 20-year period. All surgical cases were performed using a purely endoscopic approach and we evaluated the impact surgical experience on clinical outcomes. We assessed biochemical remission rates immediately following surgery (within 2 weeks of surgery), at 3 months and at the patient’s most recent follow-up appointment and analyzed predictors of successful remission in our patient group. For those who did not achieve biochemical remission, we detail the treatment course of patients placed under surveillance and those who underwent adjuvant therapy. In doing so, we illustrate a complete picture of the surgical outcomes and subsequent management of an unselected population that may be encountered during the treatment of patients with CD at a dedicated regional center.
Methods
Study Population
We analyzed the medical records of all patients diagnosed with CD who underwent primary surgical treatment at King’s College Hospital, London, between January 2004 and January 2025. Patients were identified from our prospective pituitary multidisciplinary database and cross-referenced with data from the hospital’s clinical coding department and operative database.
Preoperative Investigations
Serum cortisol was measured by chemiluminescent assay (Siemens ADVIA Centaur XP) with a sensitivity of 0.0362 nmol/L. A diagnosis of Cushing syndrome was confirmed by a serum cortisol measurement of >50 nmol/L after administering a 1-mg low-dose dexamethasone suppression test. Additional 24-hour urinary free cortisol measurements (>50 μg/24 hours), late night salivary cortisol measurements (>4 nmol/L), plasma adrenocorticotrophic hormone levels (pg/mL), and 48-hour 2-mg low-dose dexamethasone suppression tests were performed as required. All patients with confirmed Cushing syndrome underwent magnetic resonance imaging (MRI) of the pituitary gland and in equivocal cases patients also underwent corticotrophin-releasing hormone stimulation, high-dose dexamethasone suppression test, and/or inferior petrosal sinus sampling before proceeding to surgery.
Surgical Procedure
Surgery was performed via an endoscopic transnasal transsphenoidal approach in all study patients as described by Jho9 and Cappabianca.10 Image guidance was used in patients with complex or atypical sinus or vascular anatomy, those with very small microadenomas, and in patients undergoing repeat surgery. Complete hypophysectomy (sellar clearance) was performed for patients with MRI-negative Cushing disease. The histological pseudocapsular technique was employed to permit wide exposure of the sella, pituitary, and parasellar region.11,12 If a cerebrospinal fluid (CSF) leak was identified intraoperatively, an autologous adipose tissue graft was positioned in the pituitary fossa and sphenoid sinus and in selected cases a vascularized naso-septal flap was also positioned over the defect.
Postoperative Investigations and Follow-up
Our postoperative protocol included endocrinologic assessment in the early postoperative period, within 72 hours of surgery, and again within the first 2 weeks following surgery. The patient’s initial treatment strategy was defined as any surgical management within 30 days of the patient’s first surgical procedure. If a postoperative CSF leak was suspected, samples of fluid were sent for confirmatory testing of β-2-transferrin. Management of the CSF leak was determined by its severity and included observation alone, insertion of a lumbar drain and a period of bed rest, and surgical repair. Postoperative diabetes insipidus was defined as patients with polyuria requiring ongoing desmopressin therapy 6 months after surgery.
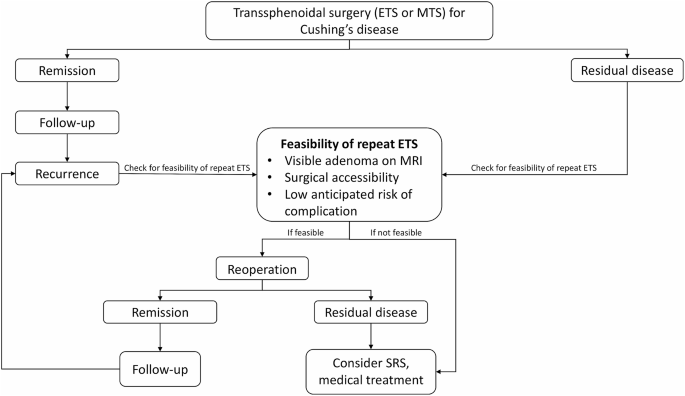
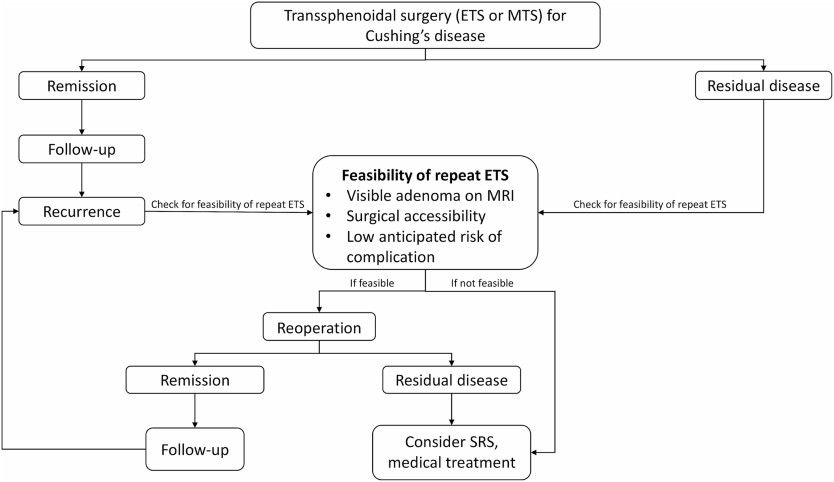
Long-term biochemical assessment of cortisol status was performed on an annual basis, or more frequently depending on the patient’s individual status. A routine postoperative MRI scan was also performed 3 months postoperatively. Remission was defined as an early morning serum cortisol of <50 nmol/L (1.8 μg/dL) requiring substitutive therapy at 3 months postoperatively. Patients who failed to enter remission were considered for further pituitary surgery, radiotherapy, medical treatment, and/or bilateral adrenalectomy. Recurrence was defined as the re-emergence of clinical features of cortisol excess supported by biochemical evidence of cortisol excess as described above. Persistent disease was defined as such was defined as a postoperative basal cortisol(s) > 50 nmol/.
Data Collection
We reviewed the biochemical, radiologic, medical, and surgical records of all study patients. The following data were collected: demographic features, preoperative endocrinologic measurements, radiologic MRI features of the tumor (including tumor visibility on MRI and size), procedural complications (including CSF leak, meningitis, diabetes insipidus [DI], hematoma, visual complications, or new cranial nerve deficits), postoperative endocrinologic assessments, and any further treatments performed.
Statistical Analysis
Categorical data are summarized using frequencies and percentages and continuous data are described using means, standard deviations, medians, and ranges. Associations between categorical variables were assessed using Fisher’s Exact test. Multivariable logistic regression models were performed in which remission statuses at (i) 3 months and (ii) last follow-up were used as outcome variables. The list of predictors of each outcome included patient characteristics (sex, age), tumor category, number of operations performed, and the presence of postoperational complications, which were decided a priori. Subgroup analyses were also performed based on tumor category—microadenomas, macroadenomas, and MRI-negative CD.
Data were collated in Microsoft Excel (Microsoft, Redmond, WA). All statistical analyses were performed using R software version 4.2.1 (R Foundation for Statistical Computing, 2022; r-project.org). P-values less than 0.05 were considered statistically significant.
Ethics Statement
This study was approved by King’s College Hospital’s research committee without the need for informed consent. The study was conducted in accordance with the ethics standards of the institution’s research committee and with the 1964 Helsinki declaration and its later amendments.
Results
Baseline Characteristics
A total of 125 patients including 93 (74.4%) female patients and 32 (25.6%) male patients were diagnosed with CD and had primary endoscopic transsphenoidal surgery during the study period. The median age was 48 years (range: 14–79 years). Fifty-seven patients (45.6%) had a microadenoma, 41 (32.8%) had a macroadenoma, and 26 (20.8%) had no demonstrable focal lesion on pituitary MRI (MRI-negative CD). The median length of follow-up was 3.1 years (range: 1 month to 16.7 years). Of the 125 patients included in our study, 88 patients (70.4%) had a single operation during their initial treatment strategy. Thirty-seven patients (29.6%) had more than 1 operation; 4 patients (3.2%) had 3 operations during the study period. A summary of the baseline characteristics of our patients can be found in Table 1.
Table 1. Baseline Characteristics of the Study Population
| Number of Patients | 125 |
|---|---|
| Patient variables | |
| Age | Median 48 (range: 14–79) years |
| Male | 32 (25.6%) |
| Pituitary characteristics | |
| Microadenoma | 57 (45.6%) |
| Macroadenoma | 41 (32.8%) |
| No focal lesion on pituitary MRI (MRI-negative Cushing’ disease) | 26 (20.8%) |
| Operative variables | |
| Single operation | 88 (70.4%) |
| More than 1 operation | 33 (26.4%) |
| 3 operations | 4 (3.2%) |
Perioperative Complications
Forty patients (32.0%) had a complication following their surgery (Table 2). The overall complication rate for patients undergoing a single procedure was 23.9% (21 of 88) and was significantly lower than the complication rate in patients who had multiple operations: 51.3% (19 of 37) (P = 0.002). The complication rates for different tumor types were not significantly different: microadenoma 33.3% (19 of 57), macroadenoma 36.6% (15 of 41), MRI-negative CD 23.1% (6 of 26) (P = 0.274). There was a significant difference between complications in the second period; Period 1: 8.7% (2 of 23) and Period 2: 37.3% (38 of 102) (P = 0.008).
Table 2. Procedural Complications Encountered in Our Series
| Complication | N (%) |
|---|---|
| Any complication | 40 (32.0%) |
| Persistent diabetes insipidus | 18 (14.4%) |
| Cerebrospinal fluid leak | 17 (13.6%) |
| Meningitis | 2 (1.6%) |
| Ventriculitis | 1 (0.8%) |
| Bleeding/haematoma | 4 (3.2%) |
| Visual deterioration | 2 (1.6%) |
| Death | 3 (2.4%) |
Eighteen patients (14.4%) developed persistent DI following surgery (requiring treatment for more than 6 months which we considered as a complication). Separately, in 12 patients (9.6%) the DI was transient and resolved spontaneously within 6 months of surgery, and 34 patients (27.2%) recovered from transient DI before discharge.
A confirmed postoperative CSF leak occurred in 17 patients (13.6%) and was significantly higher in patients who had multiple procedures; the CSF leak rate was 16.2% (6 of 37) in patients who had multiple procedures versus 12.5% (11 of 88) in those who only had a single procedure (P = 0.004). The type of tumor did not affect the CSF leak rate (P = 0.737). In 3 (2.4%) patients, the leak settled with observation alone. Three (2.4%) patients were managed with only a lumbar drain and 11 (8.8%) patients underwent surgical repair either as an executive decision or after failed lumbar drain. There were 2 (1.6%) cases with new cranial nerve deficits following surgery presenting with visual deterioration and a partial sixth nerve palsy. Two patients developed meningitis (1.6%), 1 (0.8%) developed ventriculitis. Four patients (3.2%) developed postoperative bleeding or hematoma requiring surgical attention.
Three (2.4%) patients died in the immediate perioperative period. One (0.8%) patient developed acute respiratory failure and suffered a cardiac arrest. Significant intraoperative bleeding was encountered in the other 2 cases (1.6%); 1 (0.8%) subsequently died of acute cardiorespiratory instability and the other (0.8%) died because of multiorgan failure following a prolonged stay on the intensive care unit.
Disease Remission
The overall remission rate 2 weeks following surgery was 59.0% (72 of 122), increasing to 60.7% (74 of 122) at 3 months. The remission rate 3 months following surgery was 72.0% (18 of 25) for patients with MRI-negative CD, 77.2% (44 of 57) for microadenomas, and 48.7% (19/39) for macroadenomas. Following adjuvant treatment and further surgery, the overall remission rate at last follow up was 68.0% (85 of 125).
Age, patient sex, tumor category and the number of operations were significant predictors of remission at three months. Age (adjusted odds ratio [aOR]: 1.04, 95% CI: 1.01–1.07, P = 0.009), male sex (aOR: 4.15, 95% CI: 1.64–10.53, P = 0.003), MRI-negative CD (aOR: 2.25, 95% CI: 1.24–4.07, P = 0.008), and single operation (aOR: 3.87, 95% CI: 1.56–9.61, P = 0.004), were predictors of remission at 3 months (Table 3).
Table 3. Multivariable Logistic Regression for Predictors of Remission at Last Follow-up
| Outcome | Predictor | Multivariable Analysis | |
|---|---|---|---|
| Adjusted OR (95% CI) | P Value | ||
| Remission at 3 months | Age | 1.04 (95%CI: 1.01–1.07) | 0.009 |
| Sex† | 3.31 (95%CI: 1.31–8.40) | 0.011 | |
| MRI-negative Cushing disease‡ | 1.88 (95%CI: 1.06–3.35) | 0.031 | |
| Single operation§ | 3.87 (95%CI: 1.56–9.61) | 0.004 | |
| Remission at last follow-up | Age | 1.00 (95%CI: 0.97–1.04) | 0.904 |
| Sex† | 2.92 (95%CI: 0.89–9.62) | 0.003 | |
| MRI-negative Cushing disease‡ | 1.84 (95%CI: 0.89–3.79) | 0.008 | |
| Single operation§ | 1.24 (95%CI: 0.36–4.24) | 0.730 | |
| Remission at 3 months∗ | 27.0 (95%CI: 8.47–83.33) | <0.001 | |
- ∗
-
No remission is used as the reference group.
- †
-
Female is used as the reference group.
- ‡
-
Microadenoma is used as the reference group.
- §
-
Multiple operation is used as the reference group.
Additionally, patients were more likely to be in remission at last follow-up if they had achieved remission at 3 months, compared with those who had not (aOR: 31.25, 95% CI: 11.2–90.9, P < 0.001). On multivariable analysis, this remained significant (aOR: 27.0, 95% CI: 8.47–83.33, P < 0.001).
Of the 72 patients who entered remission following surgery, 5 patients (6.9%) had relapsed at their last follow-up. Further intervention was performed/planned in all patients exhibiting recurrence, including repeat surgery and radiotherapy. Four of the 5 recurrences (80.0%) happened within the first 5 years.
Growth Hormone Replacement Therapy
In total, 48.0% (60 of 125) and 40.8% (51 of 125) patients required growth hormone replacement therapy at three months and at last endocrine follow up. Nine (15.0%) patients who initially needed growth hormone replacement, no longer required it at last endocrine follow-up.
Secondary Intervention
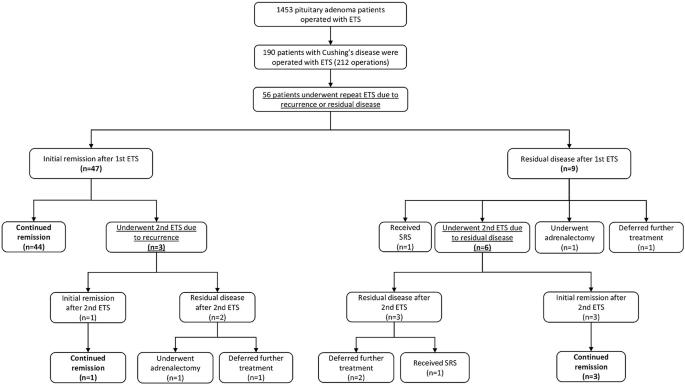
Patients with persistent disease are very likely to require a secondary intervention within a short time after initial surgery. The rate of secondary endoscopic transsphenoidal surgery was more common in patients with persistent disease (22 of 53, 41.5%) than those in initial remission (15 of 72, 20.8%) (aOR: 3.52, 95% CI: 1.48–8.38, P = 0.004). The ongoing management of patients with active disease with was tailored to the patient and included medical therapy with metyrapone, chemotherapy (temozolamide), bilateral adrenalectomy, and radiotherapy; either alone or in combination.
DISCUSSION
In one of the largest modern series in the literature, we reviewed the treatment pathway and long-term outcomes of consecutive patients treated for CD at a single regional treatment center over a 20-year period. Several previous studies have examined the surgical outcomes of patients undergoing microscopic surgery and a recent meta-analysis compared the early clinical outcomes of patients undergoing endoscopic surgery.7 However, there remains little evidence concerning the optimal long-term management of CD patients who do not immediately enter remission following surgery. Given the potential complications of CD and the challenges in managing recurrent disease, our center considers treating any patient with a cortisol of >50 nmol/L (1.8 μg/dL).
Remission
A postoperative cortisol of <50nmol/L is a good predictor of remission but not a guarantee and patients should be advised accordingly. The most conclusive finding of our study was that patients who achieved remission at 3 months were 3 times as likely to still be in remission at their last follow-up, having accounted patient and tumor characteristics. The overall initial 3-month remission rate for patients in our series was 60.7% and is comparable to other studies that have used a similarly low early morning serum cortisol level of <50 nmol/L (1.8 μg/dL) to define remission.13, 14, 15 Despite this, patients achieving early remission remain at risk of relapse with a 5-year recurrence rate of 6.9%. In addition, those with persistent disease are very likely to require a secondary intervention within a short time after initial surgery.
Using an early morning serum cortisol level of 50 nmol/L(1.8 μg/dL). to define remission enabled us to label a subgroup of patients with moderately lowered cortisol levels (50–150 nmol/L [1.8–5.4 μg/dL]) that were placed under close surveillance. It has been demonstrated that patients with postoperative cortisol of 55–137nmol/L (equivalent to 2–5.4 μg/dL) have a higher risk of late recurrence.12 We considered patients with a cortisol of greater than 150 nmol/L to be candidates for early secondary intervention without delay.
Radiotherapy, delivered by conventional external beam radiotherapy or via stereotactic radiosurgery, is typically used as a second-line treatment in CD patients after failure of initial or repeat pituitary surgery.8 In other centers, patients with similar moderately lowered cortisol level would have been labeled as being in remission and would not have been offered adjuvant radiotherapy. However, by closely observing the biochemical trends of these patients in the months following surgery we were able to offer further intervention at an earlier stage, thus avoiding the potentially harmful sequelae of untreated CD. In future work, it would be helpful to compare the long-term clinical outcomes of patients with moderately lowered serum cortisol levels who received early adjuvant therapy with patients who had similar biochemical results but did not receive adjuvant treatment.
Finally, we observed a statistically and clinically significant association between patient sex and tumor type on remission—a finding not previously reported. The underlying reasons for this result are unclear but further work should examine if, and how, the biology and histologic characteristics of adenomas changes with sex and age.9,16, 17, 18
Complications
Previous studies elected not to report the overall complication rate, hence at first sight, our overall complication rate of 32.0% may appear high even though the rate of individual specific complications are similar to those previously reported (Table 2).7, 8,15, 19 Postoperative complications were significantly higher in patients who underwent more procedures.
The overall perioperative mortality rate of 2.4% (n = 3) observed in this series is comparable with other published studies.7,8 One patient developed acute respiratory failure in the early postoperative period and died on day 3 following surgery. In the other cases significant intracavernous and intracranial bleeding was encountered and controlled; one patient subsequently developed acute cardiorespiratory instability and died on day 5; the other developed multiorgan failure and died following a prolonged stay on the intensive care unit. Following an internal review of these deaths we lowered our threshold for giving preoperative medical treatment such as ketoconazole or metyrapone in potential high-risk cases, particularly in those patients presenting with more severe clinical features at diagnosis. Preoperative medical treatment improves the quality of the tissues and increases the patient’s physiological reserve in preparation for surgery.14 In the ERCUSYN study, patients with severe clinical features who were treated preoperatively experienced comparable outcomes to those patients with milder features who were not treated with medical treatment before surgery. This justifies our approach to treat the more severe cases medically in the first instance. Nevertheless, preoperative medical treatment may confound the interpretation of early postoperative serum cortisol levels so close monitoring of these patients is required in the first few months following surgery.14 Since this change in practice, no deaths have occurred in patients undergoing surgery for CD at our unit.
Limitations
CD is a rare disease, and this study offers one of the larger modern series with practical illustrations of multidisciplinary practice at a tertiary pituitary center. Despite its size, this study did confirm that patients who achieved remission at 3 months were more likely to be in remission at the last follow-up. Patient and tumor characteristics were also important factors to consider. This study is nonetheless limited by lack of data on residual tumors found in postoperative MRIs. As such, we were unable to investigate further on the subgroup of patients without biochemical remission who had residual tumors. Furthermore, we do not fully know the proportion of MRI-negative patients who harbored an adenoma on histopathology, which may have skewed our findings. Further multi-institutional research is required to determine if patients with moderately lowered serum cortisol levels who receive early adjuvant radiotherapy have improved long-term clinical outcomes.
Conclusions
Despite good initial remission rates following endoscopic transsphenoidal surgery, this study demonstrated significant recurrence of CD. Nevertheless, patients who achieved initial biochemical remission (serum cortisol <50 nmol/L [1.8 μg/dL]) at 3 months were significantly more likely to achieve long-term biochemical remission. Selected patients with moderately lowered serum cortisol (serum cortisol 50–150 nmol/L [1.8–5.4 μg/dL]) responded well to early adjuvant radiotherapy but further research is required to determine their long-term clinical outcomes.
CRediT authorship contribution statement
Jonathan Shapey: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. Keng Siang Lee: Data curation, Formal analysis, Visualization, Writing – original draft. Vanitha Karunakaran: Formal analysis, Visualization, Writing – review & editing. Mohamed Okasha: Data curation, Writing – review & editing. Proma Dey: Data curation. Sabina Pate: Data curation. Mariusz T. Grzeda: Formal analysis, Writing – review & editing. Jackie Gilbert: Data curation, Writing – review & editing. Paul V. Carroll: Data curation, Writing – review & editing. Benjamin Whitelaw: Data curation, Writing – review & editing. Konstantinos Barkas: Data
-
Cushing disease over 50 years in Stoke-on-Trent, UK: audit and meta-analysis of literatureJ Clin Endocrinol Metab, 96 (2011), pp. 632-642
- 2
J. Etxabe, J.A. VazquezMorbidity and mortality in Cushing disease: an epidemiological approachClin Endocrinol (Oxf), 40 (1994), pp. 479-484
- 3
O. Ragnarsson, D.S. Olsson, D. Chantzichristos, et al.The incidence of Cushing disease: a nationwide Swedish studyPituitary, 22 (2019), pp. 179-186
- 4
M. Boscaro, G. ArnaldiApproach to the patient with possible cushing’s syndromeJ Clin Endocrinol Metab, 94 (2009), pp. 3121-3131
- 5
C.M. Plotz, A.I. Knowlton, C. RaganThe natural history of cushing’s syndromeAm J Med, 13 (1952), pp. 597-614
- 6
A.B. Atkinson, A. Kennedy, M.I. Wiggam, D.R. McCance, B. SheridanLong-term remission rates after pituitary surgery for Cushing disease: the need for long-term surveillanceClin Endocrinol (Oxf), 63 (2005), pp. 549-559
- 7
L.H.A. Broersen, N.R. Biermasz, W.R. van Furth, et al.Endoscopic vs. microscopic transsphenoidal surgery for Cushing disease: a systematic review and meta-analysisPituitary, 21 (2018), pp. 524-534
- 8
R. Pivonello, M. De Leo, A. Cozzolino, A. ColaoThe treatment of cushing’s diseaseEndocr Rev, 36 (2015), pp. 385-486
- 9
H.-D. Jho, R.L. CarrauEndoscopic endonasal transsphenoidal surgery: experience with 50 patientsJ Neurosurg, 87 (1997), pp. 44-51
- 10
P. Cappabianca, A. Alfieri, E. de DivitiisEndoscopic endonasal transsphenoidal approach to the sella: towards Functional Endoscopic Pituitary Surgery (FEPS)min – Minim Invasive Neurosurg, 41 (1998), pp. 66-73
- 11
J. Jagannathan, R. Smith, H.L. DeVroom, et al.Outcome of using the histological pseudocapsule as a surgical capsule in Cushing diseaseJ Neurosurg, 111 (2009), pp. 531-539
- 12
M. Mayberg, S. Reintjes, A. Patel, et al.Dynamics of postoperative serum cortisol after transsphenoidal surgery for Cushing disease: implications for immediate reoperation and remissionJ Neurosurg, 129 (2018), pp. 1268-1277
- 13
R.A. Alwani, W.W. de Herder, M.O. van Aken, et al.Biochemical predictors of outcome of pituitary surgery for Cushing diseaseNeuroendocrinology, 91 (2010), pp. 169-178
- 14
E. Valassi, H. Franz, T. Brue, et al.Preoperative medical treatment in Cushing syndrome: frequency of use and its impact on postoperative assessment: data from ERCUSYNEur J Endocrinol, 178 (2018), pp. 399-409
- 15
L.B. Yap, H.E. Turner, C.B.T. Adams, J.A.H. WassUndetectable postoperative cortisol does not always predict long-term remission in Cushing disease: a single centre auditClin Endocrinol (Oxf), 56 (2002), pp. 25-31
- 16
P. Cappabianca, L.M. Cavallo, A. Colao, E. de DivitiisSurgical complications associated with the endoscopic endonasal transsphenoidal approach for pituitary adenomasJ Neurosurg, 97 (2002), pp. 293-298
- 17
P. Leach, A.H. Abou-Zeid, T. Kearney, J. Davis, P.J. Trainer, K.K. GnanalinghamEndoscopic transsphenoidal pituitary surgery: evidence of an operative learning curveNeurosurgery, 67 (2010), pp. 1205-1212
- 18
C. Snyderman, A. Kassam, R. Carrau, A. Mintz, P. Gardner, D.M. PrevedelloAcquisition of surgical skills for endonasal skull base surgery: a training ProgramLaryngoscope, 117 (2007), pp. 699-705
- 19
P.C. Johnston, L. Kennedy, A.H. Hamrahian, et al.Surgical outcomes in patients with Cushing disease: the Cleveland clinic experiencePituitary, 20 (2017), pp. 430-440
curation, Writing – review & editing. Eleni Maratos: Data curation, Writing – review & editing. Sinan Barazi: Data curation, Writing – review & editing. Simon Aylwin: Data curation, Methodology, Supervision, Writing – original draft, Writing – review & editing. Nick WM. Thomas: Conceptualization, Data curation, Methodology, Supervision, Writing – review & editing.
References
- 1
R.N. Clayton, D. Raskauskiene, R.C. Reulen, P.W. JonesMortality and morbidity in
Filed under: Cushing's, pituitary, Treatments | Tagged: Cushing's Disease, endoscopic, pituitary, remission, transsphenoidal | Leave a comment »